Case of the Month – November 2019
Quiz Summary
0 of 3 questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 3 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
-
 Canadian Society of Pathology
Canadian Society of PathologyCase Of The Month
Contributor:
Omar Al-Nourhji, MD, FRCPC
University of SaskatchewanGlenda Wright, MBBCh
General Pathology Resident
Department of Laboratory Medicine and Pathology
University of Saskatchewan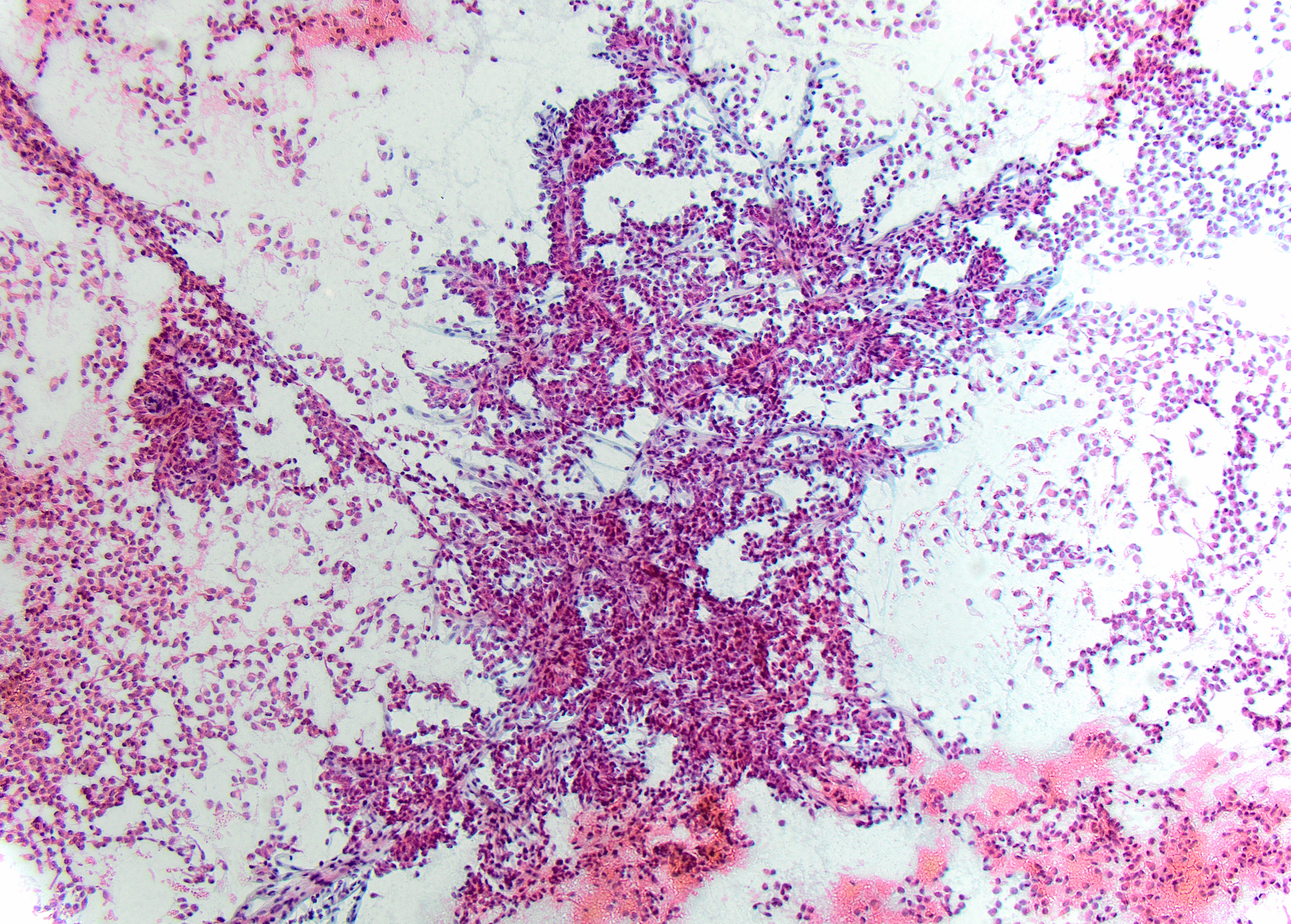
Direct smear – Pap stained x10
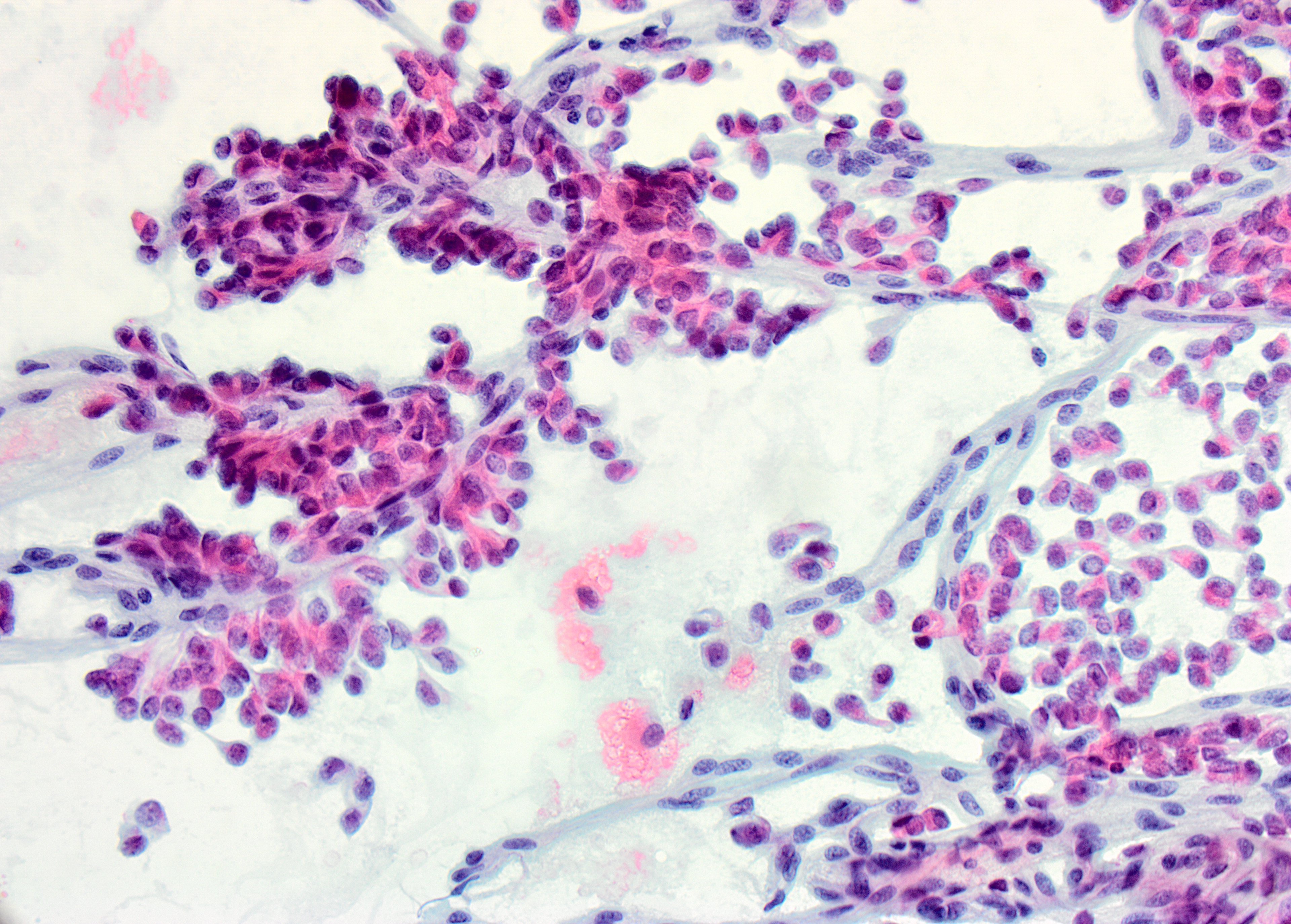
Direct smear – Pap stained x40
Canadian Society of Pathology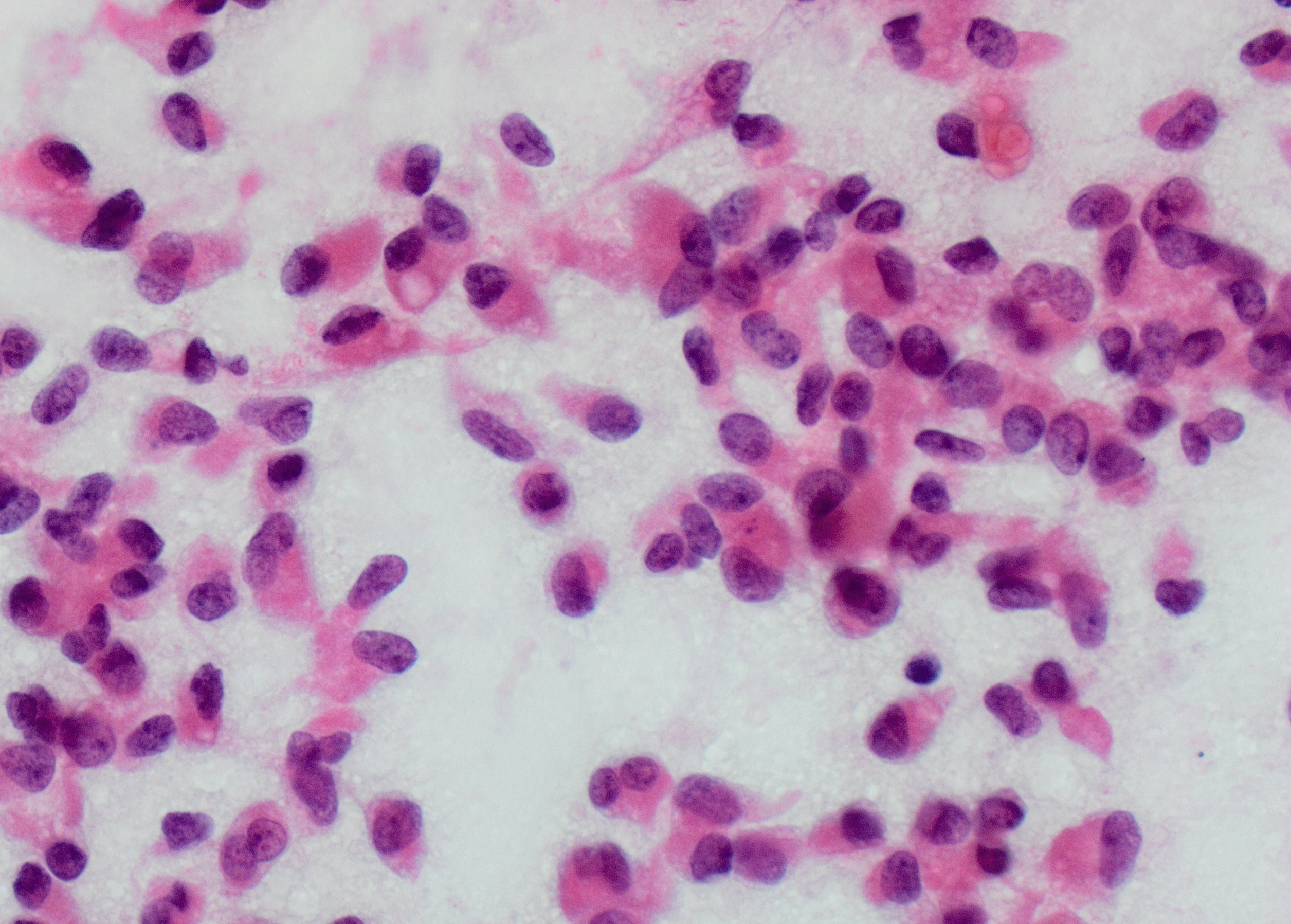
Direct smear – Pap stained x100
Discussion
Given the patient’s age, gender and cytomorphologic features shown, the most likely diagnosis is solid pseudopapillary neoplasm (SPN). Fine Needle Aspiration Cytology (FNAC) of this lesion characteristically shows cellular aspirates, consisting of a monomorphic epithelioid to plasmacytoid neoplastic cells, forming pseudopapillary structures and dispersed singularly. The pseudopapillae consist of central delicate capillaries lined by multiple layers of neoplastic cells. Neoplastic cells with long cytoplasmic wisps anchoring to the papillary cores, also known as “Cercariform cells”, have been recently described in SPN. The neoplastic cells are small, with pale to vacuolated cytoplasm, inconspicuous nucleoli, and longitudinal nuclear grooves. A degenerative background, extracellular magenta matrix, hyaline globules are additional features reported in SPN.
Pancreatic neuroendocrine tumors (Pan-NET), especially those with cystic degeneration, may resemble SPNs and are therefore the primary entity considered in the differential diagnosis. Aspirates from Pan-NETs are usually cellular, consisting of uniform, monotonous population of plasmacytoid cells with speckled, “salt-and-pepper” chromatin, finely granular cytoplasm and small to prominent nucleoli.
Pancreatic Ductal Adenocarcinoma shows disorganized honeycomb sheets of cells with greater anisonucleosis and nuclear membrane irregularity. Acinar Cell Carcinoma (ACC) aspirates would consist of isolated cells and loose aggregates with abundant granular cytoplasm and prominent nucleoli. Intraductal Papillary Mucinous Neoplasm (IPMN) typically produce hypocellular smears with background mucin and clusters of glandular cells.
Given the morphologic overlap between SPN and Pan-NETs, immunohistochemical stains are usually necessary for a definitive diagnosis. Strong positive nuclear beta-catenin staining, strong diffuse membranous and cytoplasmic CD10 staining, and intracellular and extracellular PAS positive, diastase resistant globules are specific for Solid Pseudopapillary Neoplasms. Both SPN and Pan-NET maybe positive for synaptophysin and CD56. However, Pan-NET stain positively for chromogranin, while the majority of SPN are negative for chromogranin. ACC show positive staining with pancreatic enzymes, such as trypsin and chymotrypsin, and contain PAS intracytoplasmic positive granules. Positivity for CK7, CK8/18, and p53 are in keeping with Pancreatic Ductal Adenocarcinoma.
Molecular and cytogenetic alterations are increasingly being defined for pancreatic lesions. SPN show a characteristic activating point mutation of the beta-catenin gene CTNNB1, identified in greater than 95% of tumours. This mutation prevents destruction of beta-catenin, causing relocation of the molecule to the nucleus and activation of the Wnt/beta-catenin pathway. Loss of SMAD4 is a marker of invasive adenocarcinoma. KRAS mutations and P16/CDKN2A inactivation are identified in many pancreatic ductal neoplasms, including pancreatic intraepithelial neoplasia, IPMN, and mucinous cystic neoplasms. One of the most common cytogenetic alterations found in pancreatic NET involves mutation or LOH at the MEN1 locus, both in inherited germline and sporadic tumours. Aallelic loss of 11p is reported in pancreatoblastomas.
SPNs are rare pancreatic tumours of low malignant potential. These neoplasms occur in young females and can be situated anywhere through out the length of the pancreas. The lesions are often found incidentally or present with non-specific abdominal symptoms. Grossly, a large well circumscribed solid to cystic mass is identified. On histological examination, pseudopapillary structures are identified with the same cytological features identified on FNAC. The treatment of choice is complete surgical excision and the majority of patients have a good prognosis, with only infrequent recurrence. A minority of Solid Pseudopapillary Neoplasms show aggressive features, including necrosis, high mitotic activity, infiltration into adjacent structures and metastases to other organs.
References
- Dinarvand P. Solid Pseudopapillary Neoplasm of the Pancreas. Archives of Pathology and Laboratory Medicine. 2017;141:990-995
- Policarpio-Nicolas MLC, McHugh KE, Sae-Ow W, Brainard JA. Pleomorphic and atypical multinucleated giant cells in solid pseudopapillary neoplasm of pancreas: A diagnostic pitfall in cytology and review of the literature. Diagnostic Cytopathology. 2018;Dec:1-6 [ePub ahead of print]
- Misra A, Saran RK, Srivastava S, Barman S, Dahale A. Utility of cytomorphology in distinguishing solid pseudopapillary neoplasm of pancreas from pancreatic neuroendocrine tumour with emphasis on nuclear folds and nuclear grooves. Diagnostic Cytopathology. 2019; Jan:1-10 [ePub ahead of print]
- Terris B, Cavard C. Diagnosis and molecular aspects of solid-pseudopapillary neoplasms of the pancreas. Seminars in Diagnostic Pathology. 2014;31:484-490
- Zhang L, Bluth MH, Bhalla A. Molecular Diagnostics in the Neoplasms of the Pancreas, Liver, Gallbladder, and Extrahepatic Biliary Tract. 2018 Update. Clinics in Laboratory Medicine. 2018;38(2):367-384
- Cibas ES, Ducatman BS. Cytology. Diagnostic Principles and Clinical Correlates. Fourth Edition (Elsevier Saunders, Philidelphia, 2015) p404-416
- 1
- 2
- 3
- Current
- Review
- Answered
- Incorrect
-
Question 1 of 3
1. Question
The MOST LIKELY diagnosis is:
CorrectIncorrect -
Question 2 of 3
2. Question
Which of the following immunohistochemical stain panels are expected to be POSITIVE in this condition?
CorrectIncorrect -
Question 3 of 3
3. Question
What molecular/cytogenetic alteration(s) is/are MOST CHARACTERISTIC of this lesion?
CorrectIncorrect