Quiz Summary
0 of 3 questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 3 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
-
 Canadian Society of Pathology
Canadian Society of PathologyCase Of The Month
Case and discussion contributed by: Cheng Wang, M.Sc., M. Med., B. Med., FRCPC
Associate Professor
Program Director, General Pathology Residency
Departments of Pathology and Urology
Faculty of Medicine, Dalhousie UniversityThe following images are representative of a voided urine sample. The patient is a 62 year old male who is a kidney transplant recipient due to end-stage renal disease secondary to sarcoidosis. He currently presents with increased creatinine. Patient’s donor-specific antibodies (DSA) are undetectable. PCR performed on his blood sample is negative for BK virus DNA amplification twice in a row.
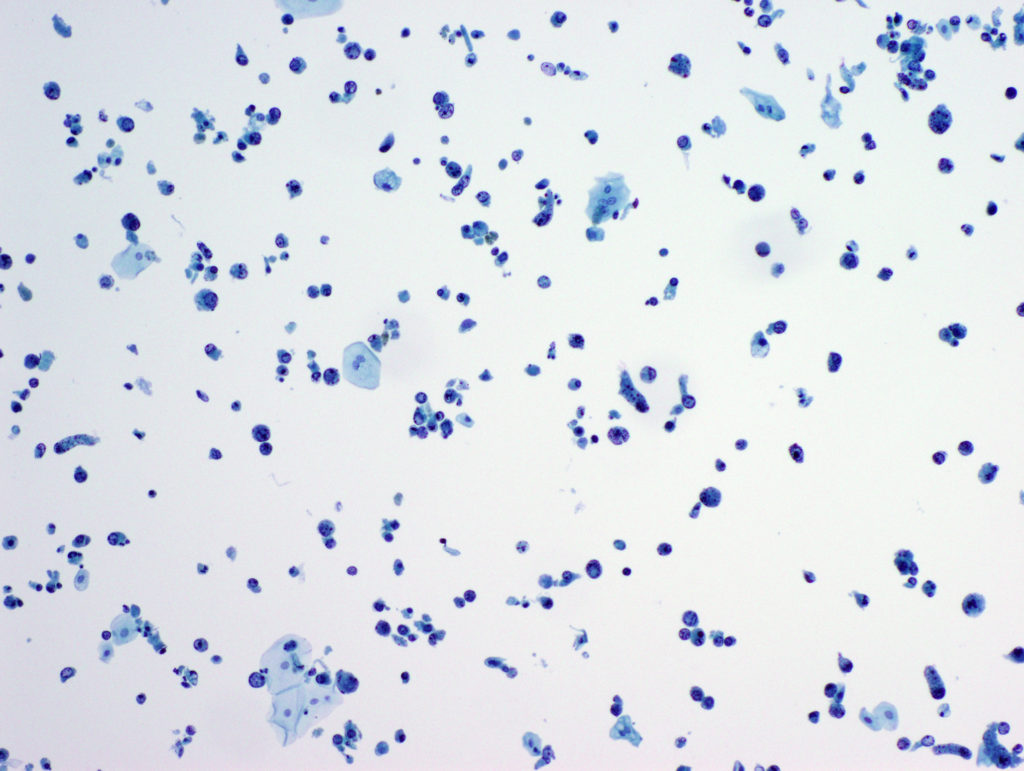
Voided urine – Liquid based cytology x10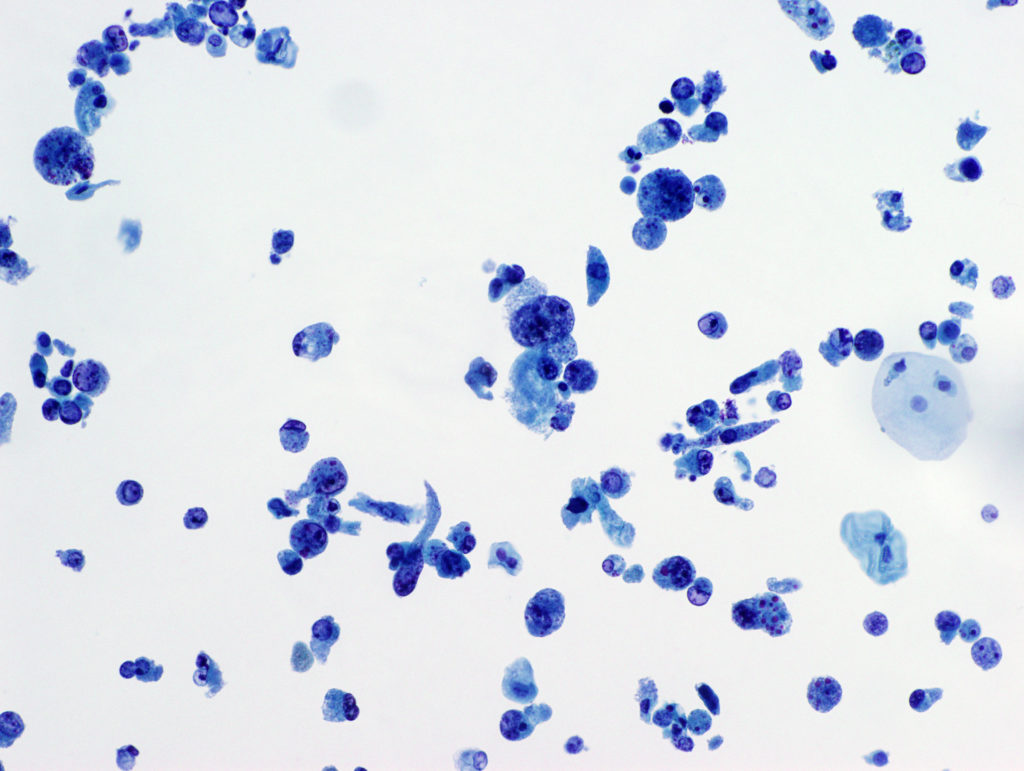
Voided urine – Liquid based cytology x20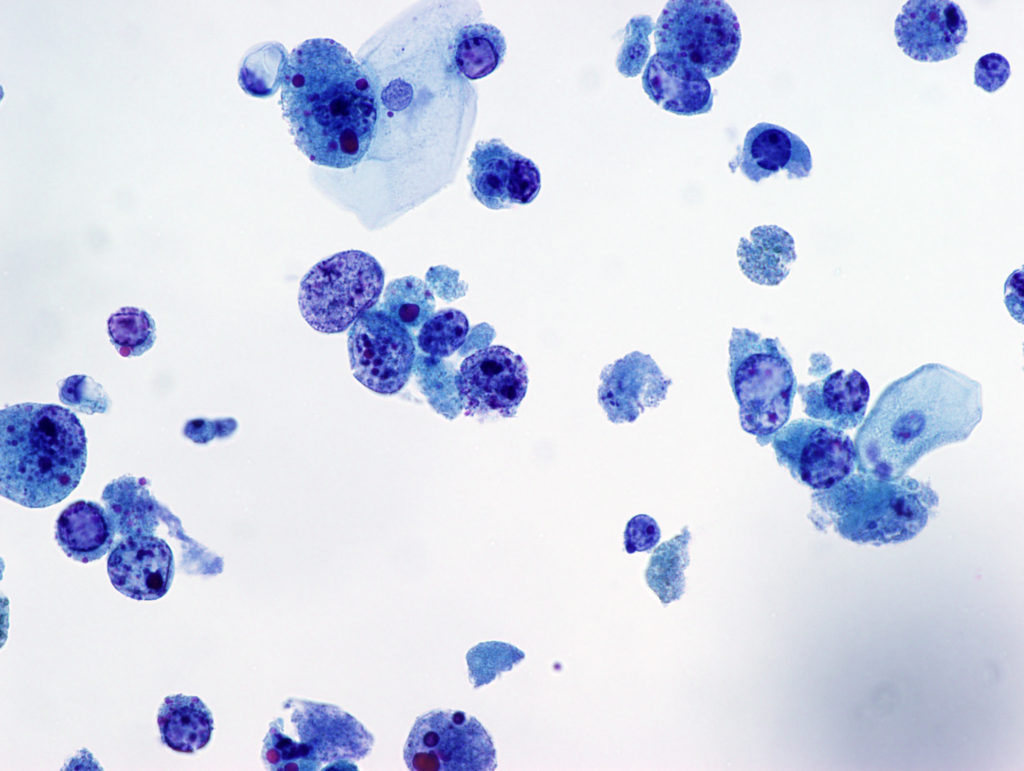
Voided urine – Liquid based cytology x40 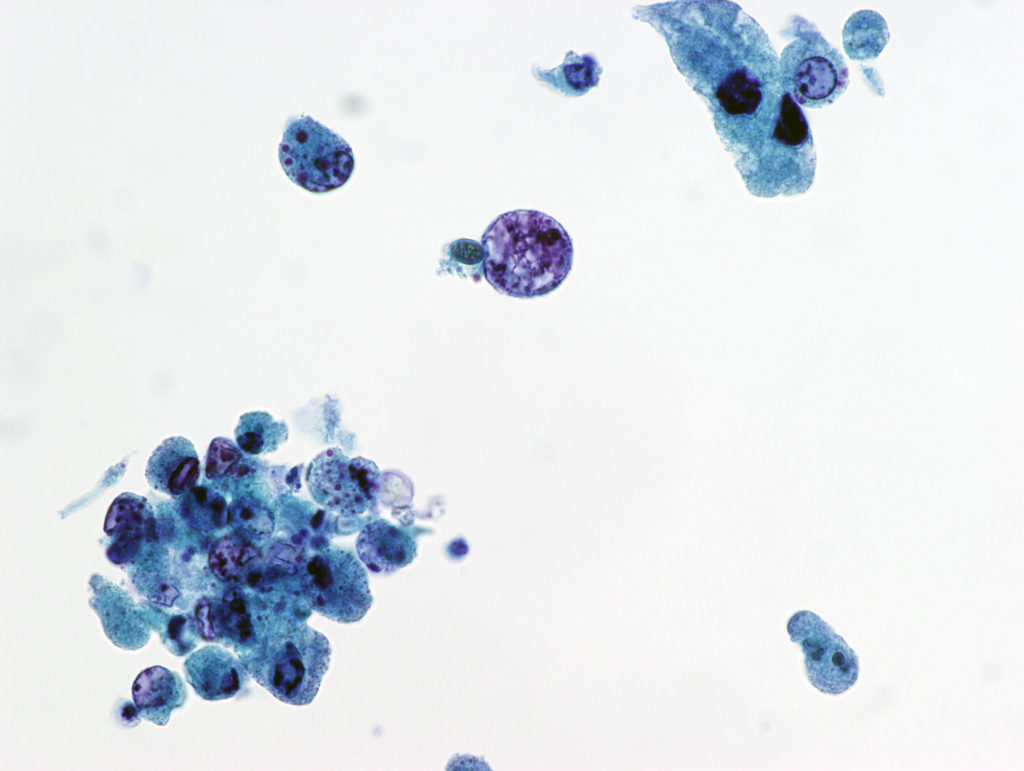
Voided urine – Liquid based cytology x40 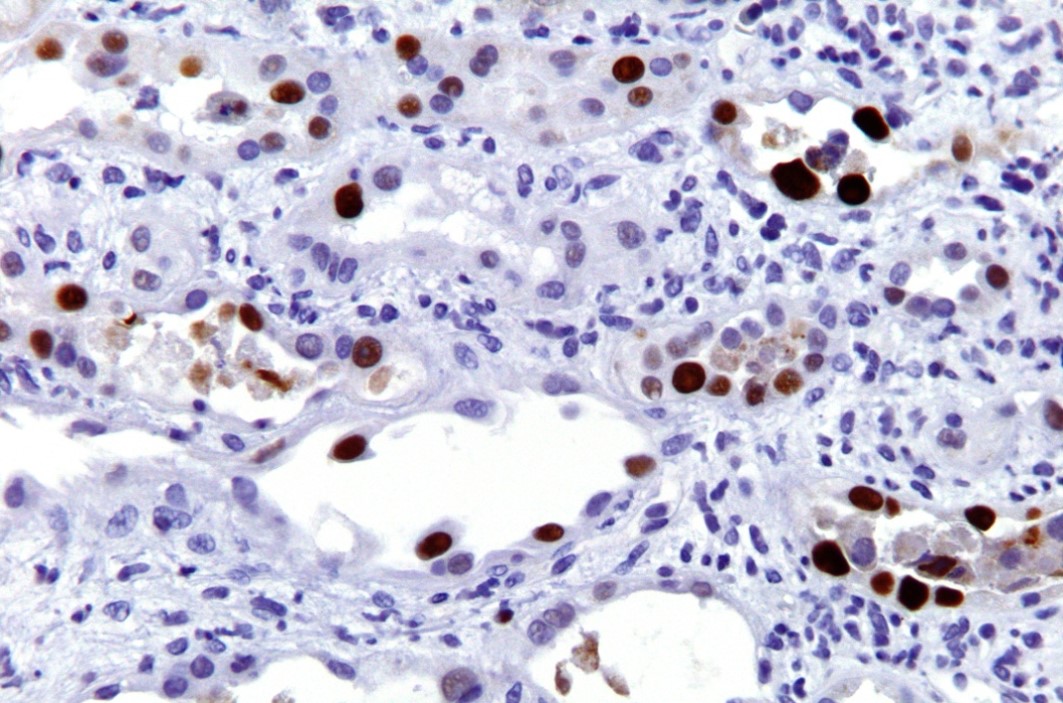
Renal biopsy – SV40 IHC – high power
.
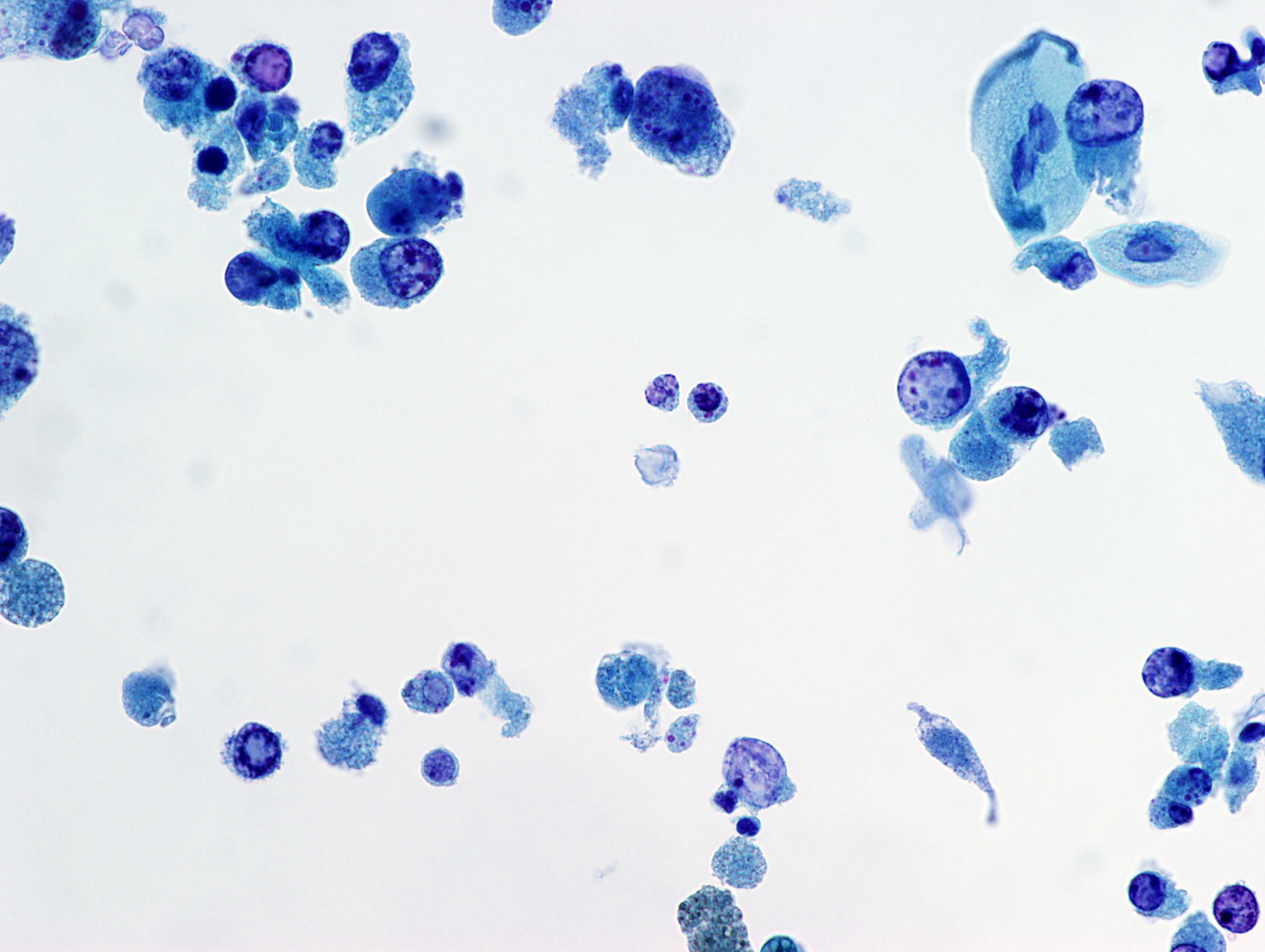
Voided urine – Liquid based cytology – Typical Polyoma virus changes x40
Discussion
BK and JC viruses are members of polyomavirus family. BK virus is associated with nephropathy and ureteral stenosis in kidney transplant patients. It is also associated with hemorrhagic cystitis in allogeneic hematopoietic cell transplant recipients. JC virus is associated with progressive multifocal leukoencephalopathy in immunocompromised patients. Both BK and JC viruses can infect urothelial cells and renal tubular cells and give rise to characteristic cytopathic effects (DeCoy cells) that can sometimes exhibit overlapping features with high-grade urothelial carcinoma. The DeCoy cells contain large, homogeneous basophilic nuclear inclusion. The nuclei of Decoy cells are generally round and smooth with ground glass appearance. DeCoy cells are generally scattered single cells without forming clusters. In our voided urine case, some DeCoy cells show scant cytoplasm and nuclei with a mild degree of membrane irregularity and coarse chromatin, reminiscent of high-grade urothelial carcinoma cells.
Although both BK and JC viruses can cause nephropathy in kidney transplant patients, there are many differences between the two. Firstly, JC virus nephropathy is not as frequent and not as well studied as the BK virus-related nephropathy in the literature. Secondly, JC virus nephropathy seems to be associated with a less aggressive and more protracted clinical course when compared with BK virus with lower rate of graft rejection and better survival. A third difference is the lower level of viremia in JC virus nephropathy in comparison to BK virus. In addition, the extent of the histological changes in JC-virus nephropathy is lower with more patchy tubular involvement and more focal cytopathologic changes.
The concurrent renal biopsy of the patient’s transplant kidney demonstrates some tubular cells with enlarged nuclei and hyperchromasia. These tubular cells also stained positive by an antibody against SV40 large T antigen, confirming the presence of polyomavirus cytopathic effects. It is noted that only a few tubules are showing cytopathic effects, which is common for JC virus infection as opposed to the more diffuse tubular cell changes related to BK virus infection. Given the results of qPCR performed on the patient’s blood, a diagnosis of JC virus nephropathy was established.
After being diagnosed with JC virus-associated nephropathy, one of the patient’s immunosuppressive agents was changed and the patient’s creatinine returned to the baseline.
In addition to BK and JC viruses, there are several relatively new members of Polyomavirus that have identified recently:
- Merkel cell polyomavirus: associated with Merkel cell carcinoma
- TS polyomavirus: associated with trichodysplasia spinulosa, a rare skin disease in immunocompromised hosts, characterized by follicular papules, keratin spines known as spicules, and alopecia
- Human polyomavirus 7: associated with a pruritic rash and viremia in lung transplant recipients.
References
(1) Drachenberg et al. Polyomavirus BK versus JC replication and nephropathy in renal transplant recipients: a prospective evaluation. Transplantation. 2007 Aug 15;84(3):323-30.
(2) Delbue S, et al. A review on JC virus infection in kidney transplant recipients. Clin Dev immunol. 2013; 2013: 926391.
(3) Hirsch. Overview of JC polyomarvirus, BK polyomavirus and other polyomavirus infections. Uptodate 2020
(4) Cibas and Ducatman: Cytology, Diagnositc Principles and Clinical Correlates. 4th Edition
- 1
- 2
- 3
- Current
- Review
- Answered
- Incorrect
-
Question 1 of 3
1. Question
The most likely diagnosis of the void urine sample is:
CorrectIncorrect -
Question 2 of 3
2. Question
The patient’s blood sample was sent out for external laboratory testing, which showed JC virus DNA amplification (2.02E+4 copies/ml by qPCR). His concurrent renal biopsy showed a few tubular cells with markedly enlarged nuclei. Which of the following antibody should be utilized to confirm the diagnosis?
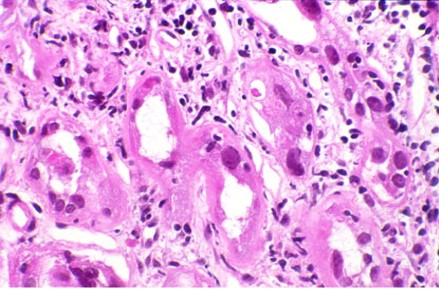
Renal biopsy – H&E stained – high powerCorrectIncorrect -
Question 3 of 3
3. Question
In addition to nephropathy, JC virus is also associated with which of the following?
CorrectIncorrect