A 60 year old female presented with a right large pleural effusion and pleuritic pain. She had a remote history of resected ovarian teratoma in 1985. Clinical impression was empyema. Right pleural fluid was sent for cytology.
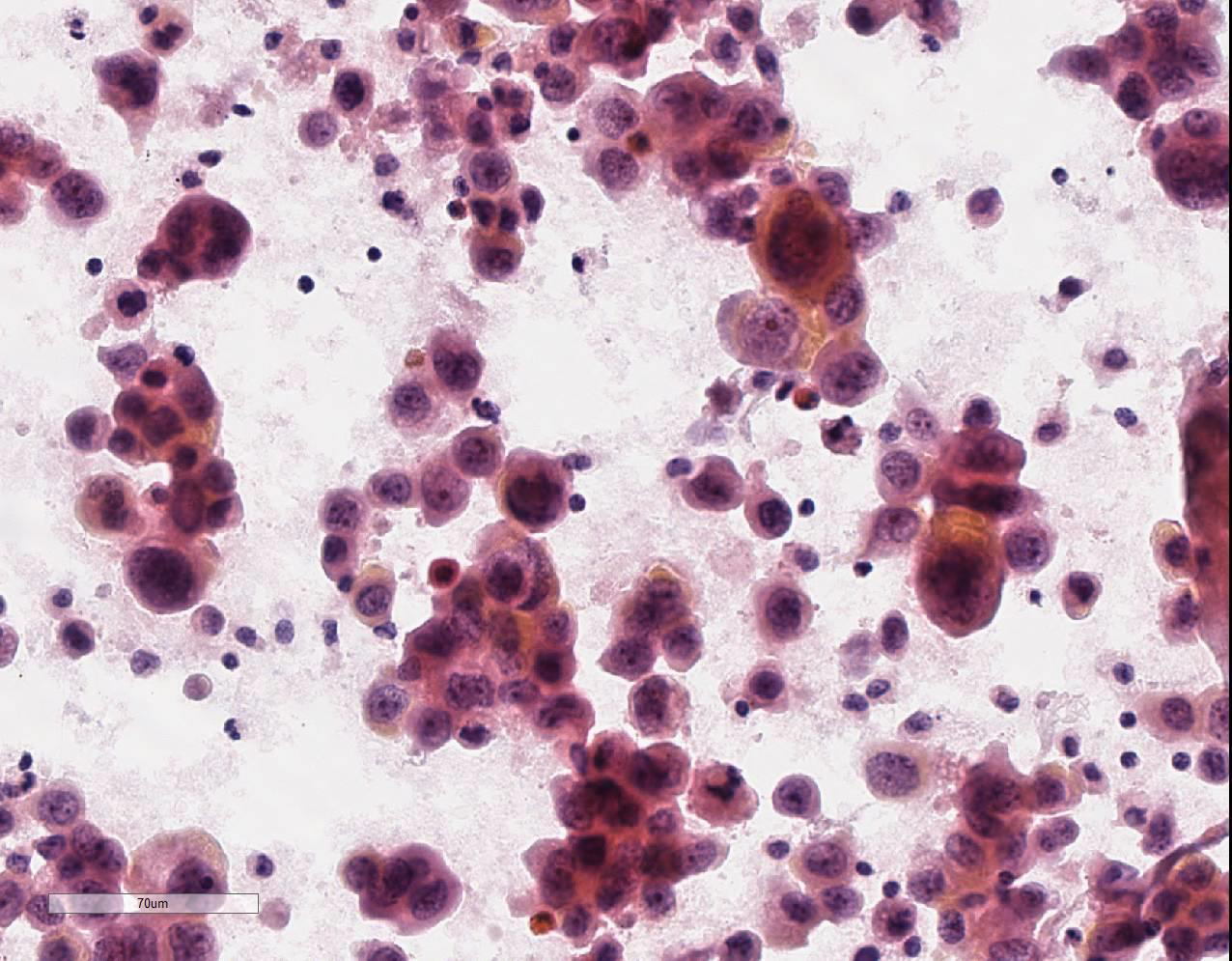
Cytopsin – High power, Pap. Stained
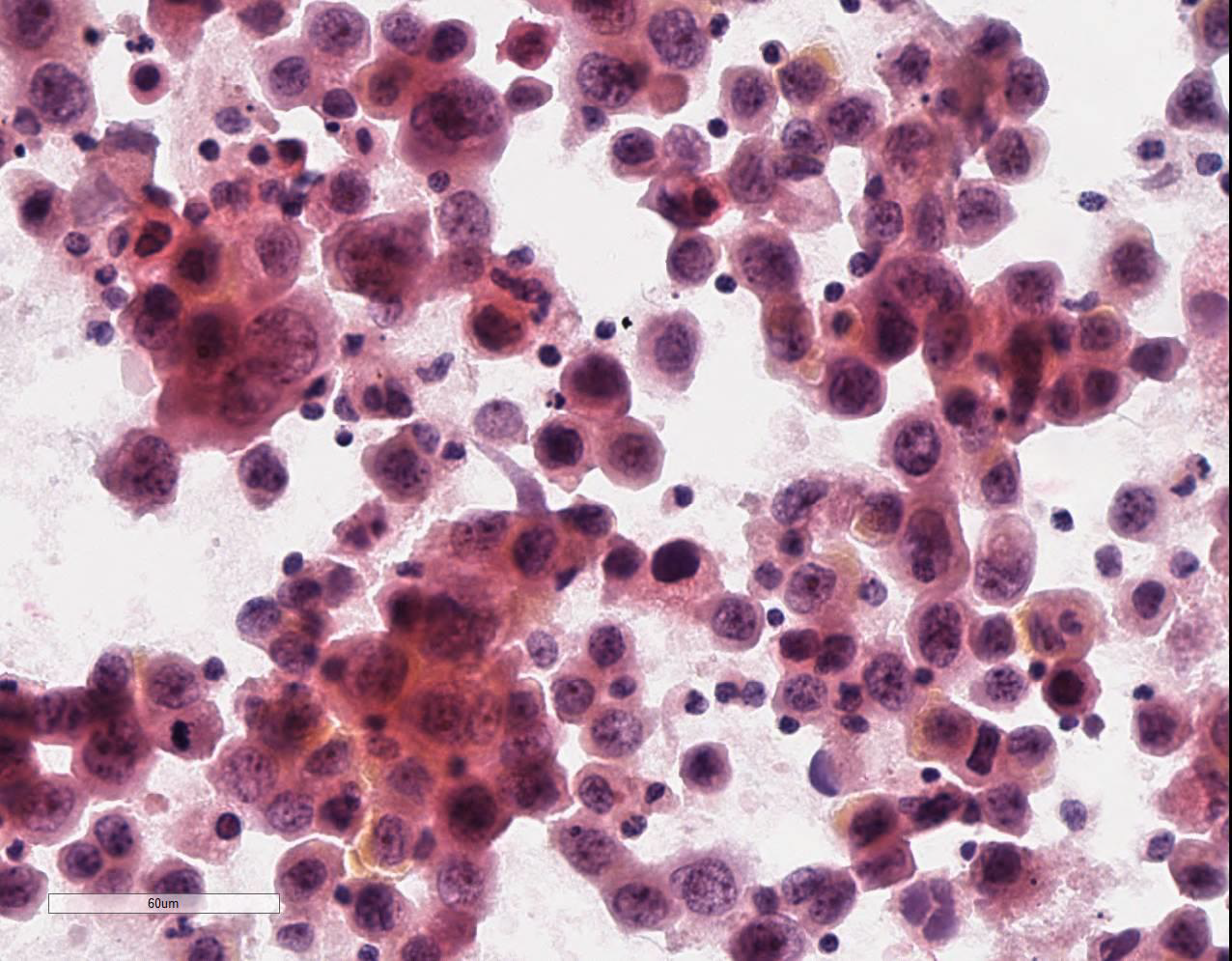
Cytopsin – High power, Pap. Stained
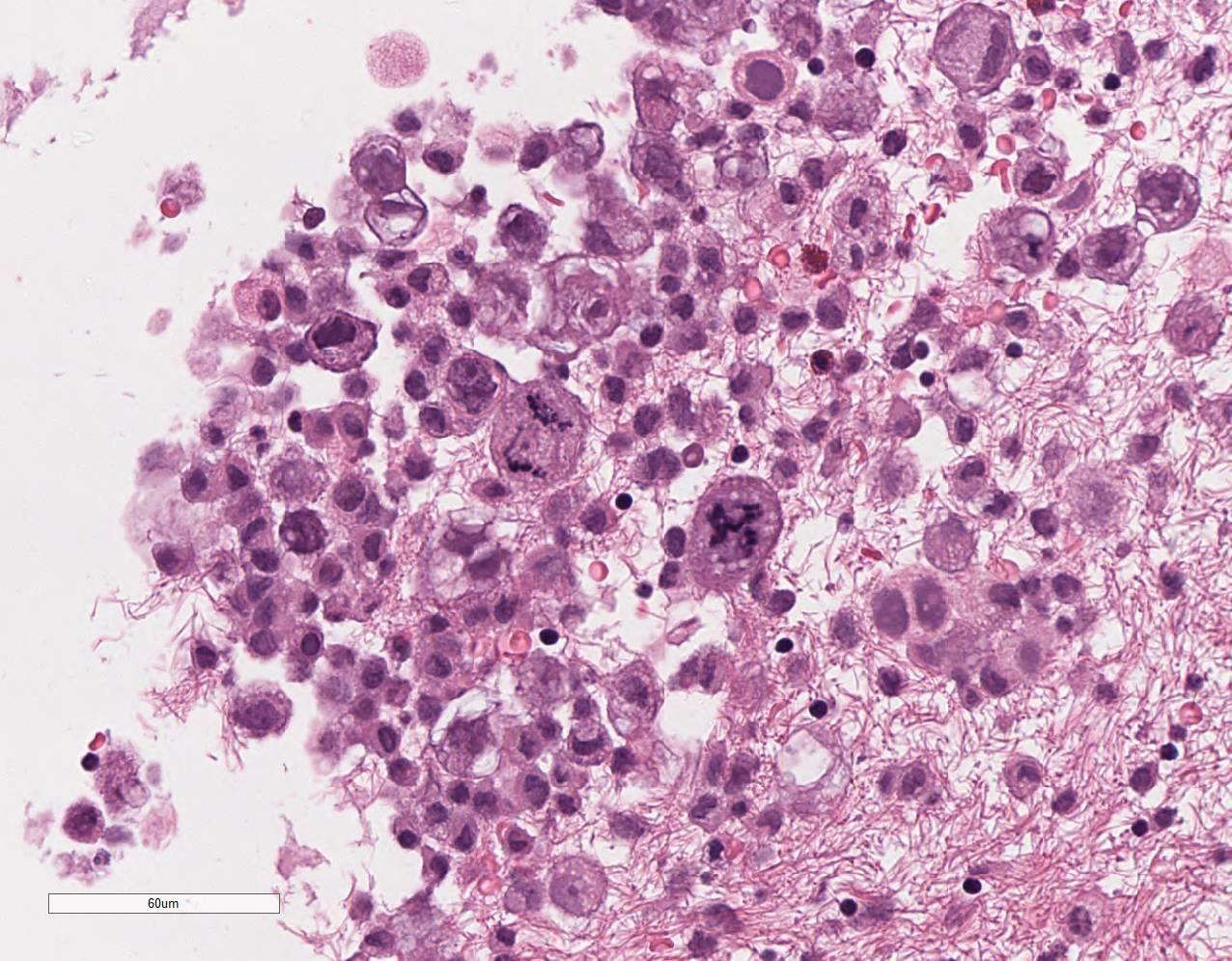
Cell block – High power, H&E
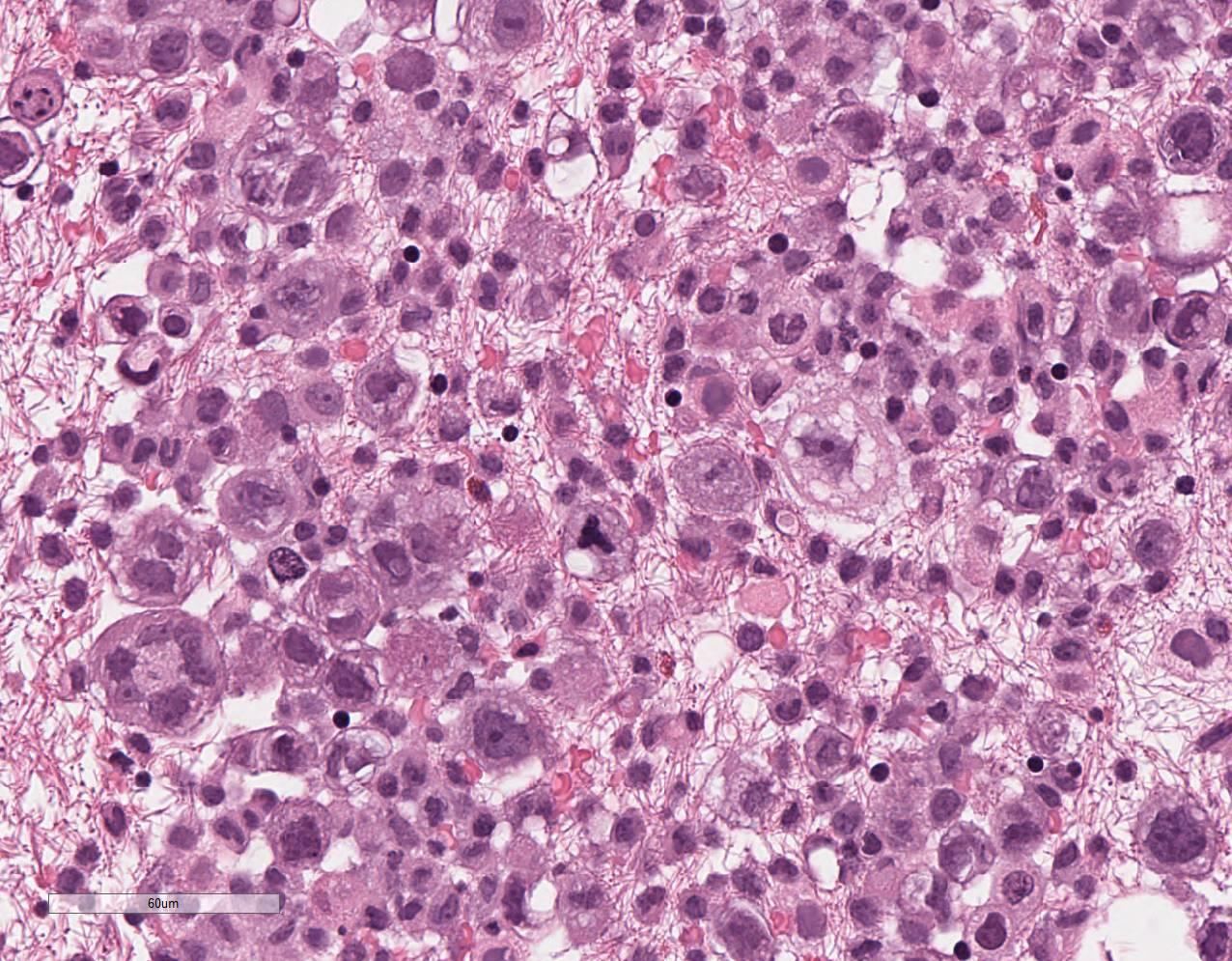
Cell block – High power, H&E

Cell block – High power, H&E
Quiz Summary
0 of 3 questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 3 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
-
 Canadian Society of Pathology
Canadian Society of PathologyCase Of The Month
Contributor: Marc Pusztaszeri, MD Associate Professor Department of Pathology McGill University
Glenda Wright, MBBCh General Pathology Resident Department of Laboratory Medicine and Pathology University of Saskatchewan
 Immunohistochemical staining for Ber-EP4 is negative
Immunohistochemical staining for Ber-EP4 is negative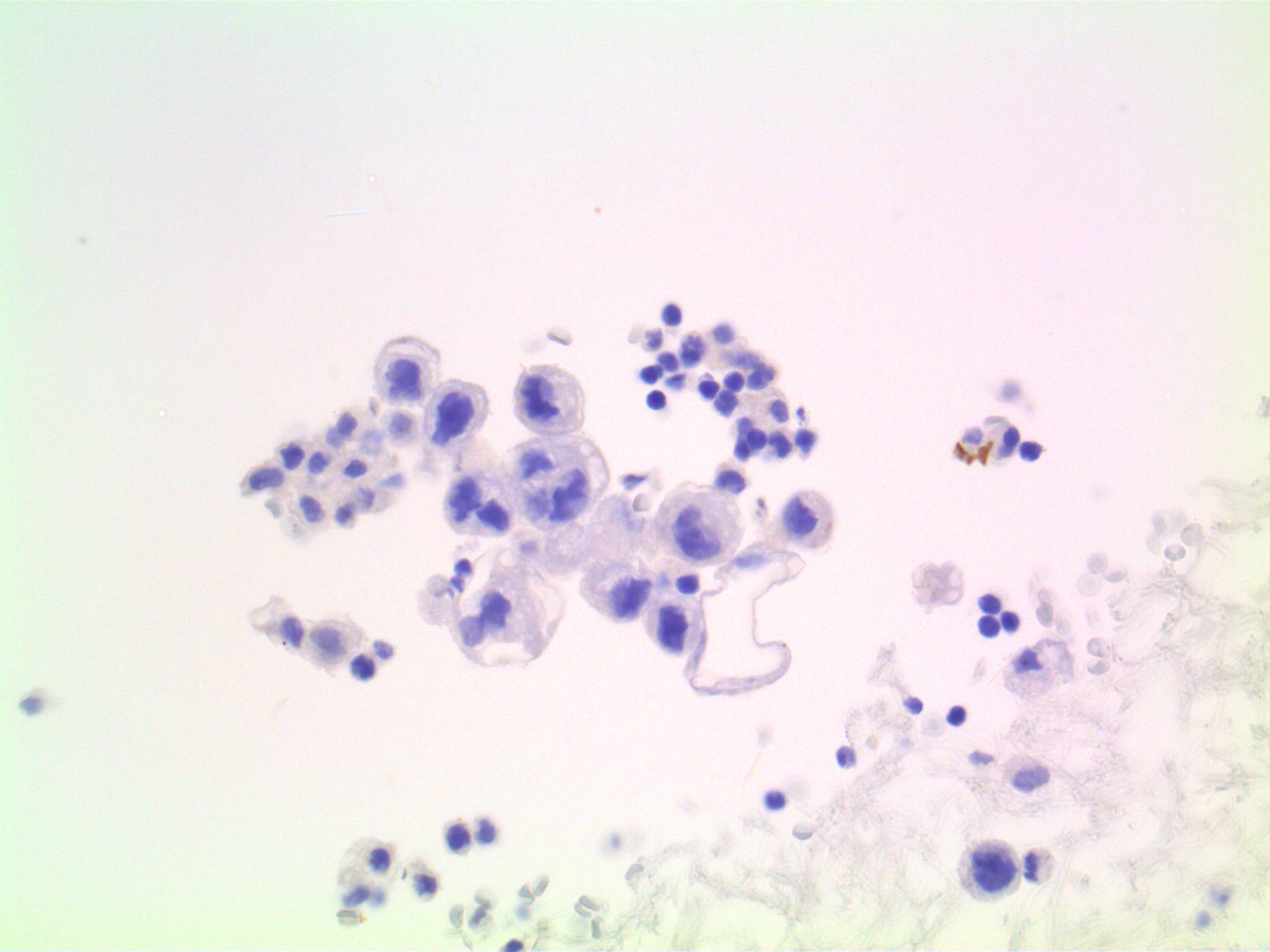 Immunohistochemical staining for MOC-31 is negative
Immunohistochemical staining for MOC-31 is negative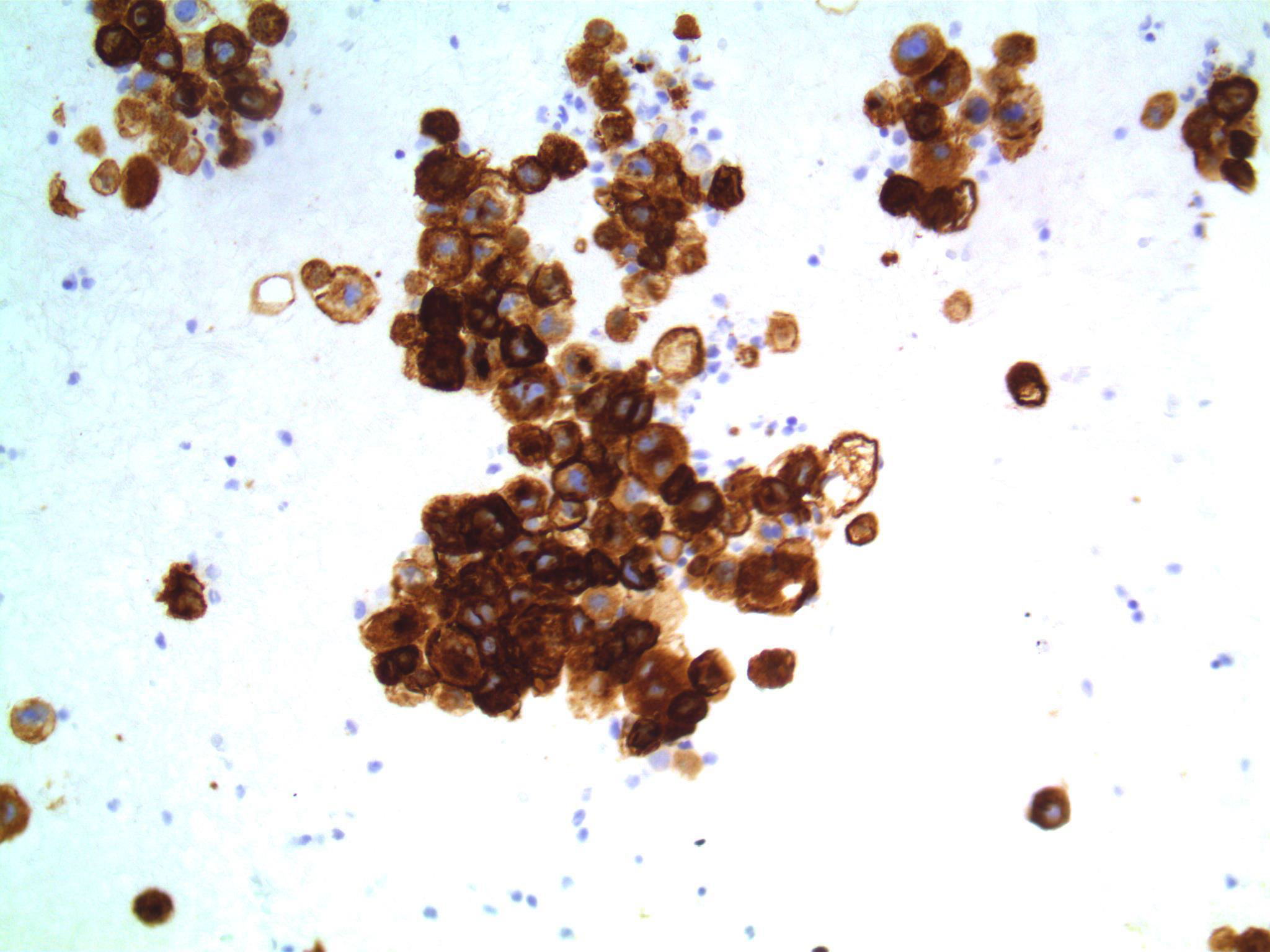 Positive immunohistochemical staining for EMA
Positive immunohistochemical staining for EMA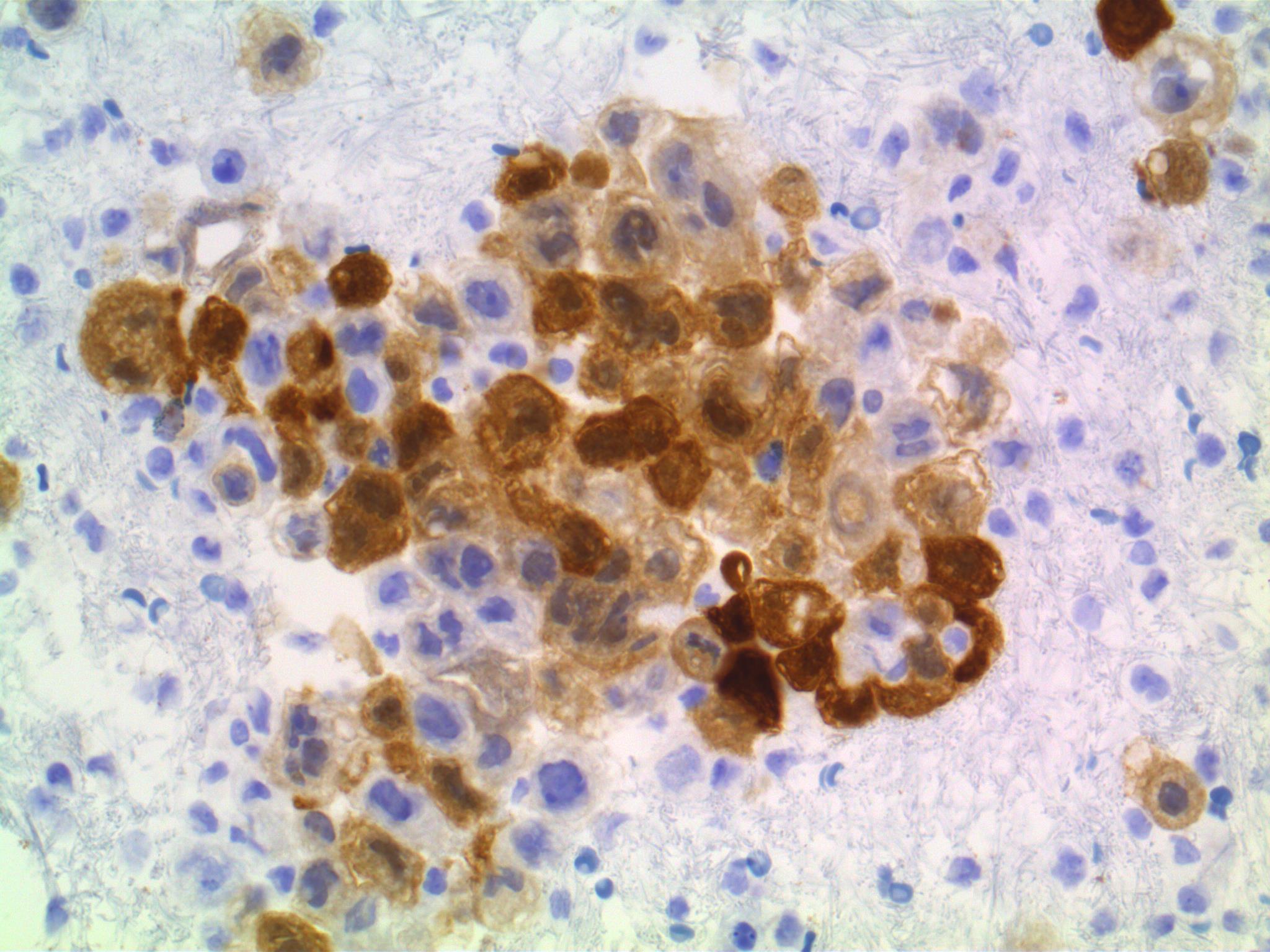 Positive immunohistochemical staining for calretinin
Positive immunohistochemical staining for calretinin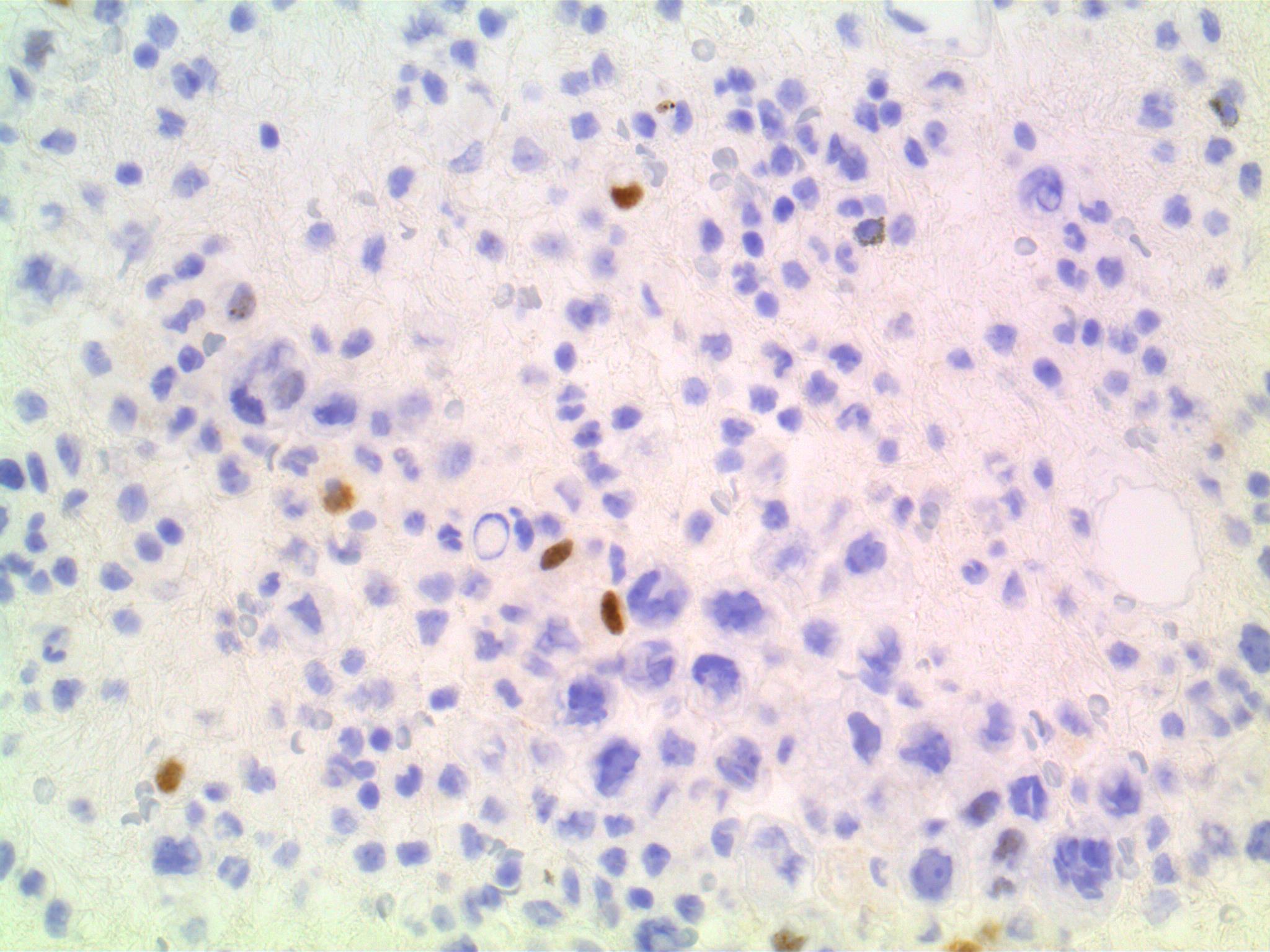 Focal positive immunohistochemical staining for WT-1
Focal positive immunohistochemical staining for WT-1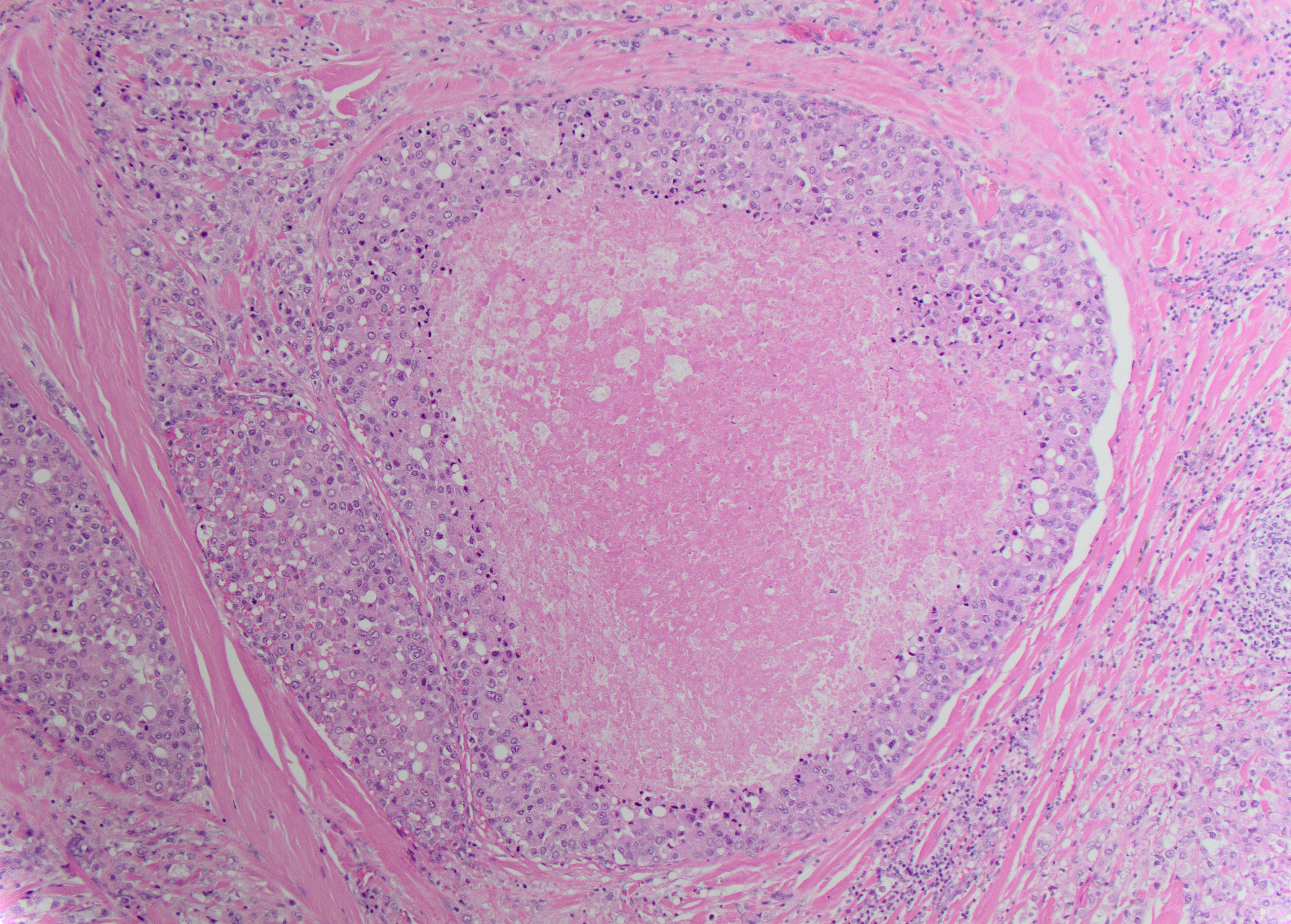 Focal positive immunohistochemical staining for D2-40
Focal positive immunohistochemical staining for D2-40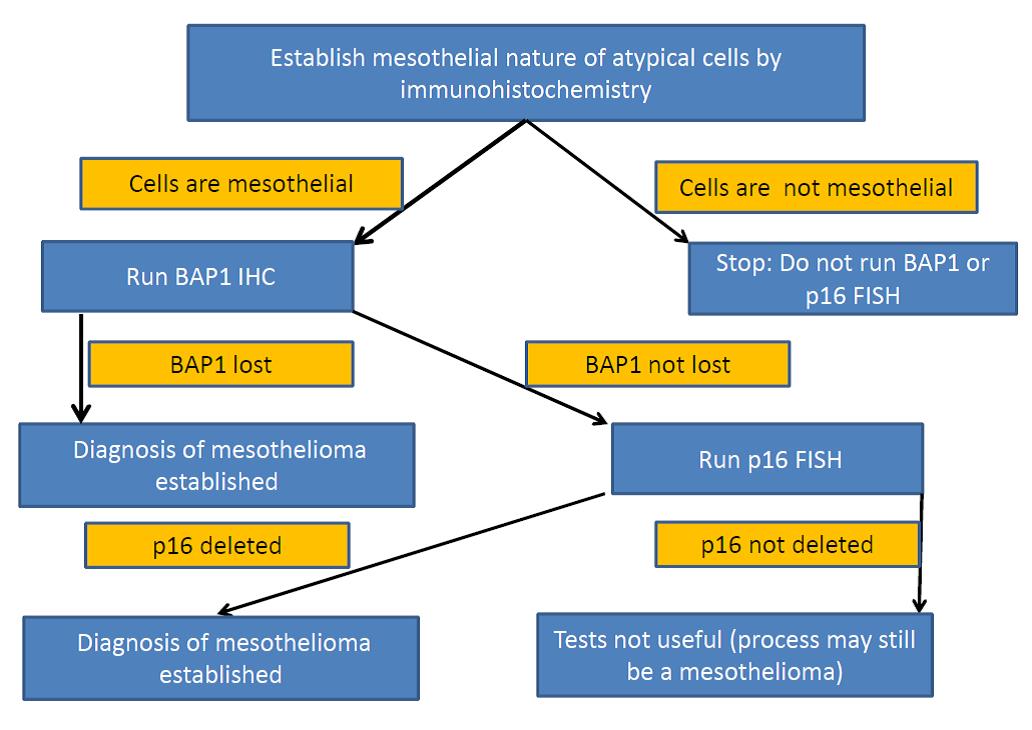 Positive immunohistochemical staining for GATA-3
Positive immunohistochemical staining for GATA-3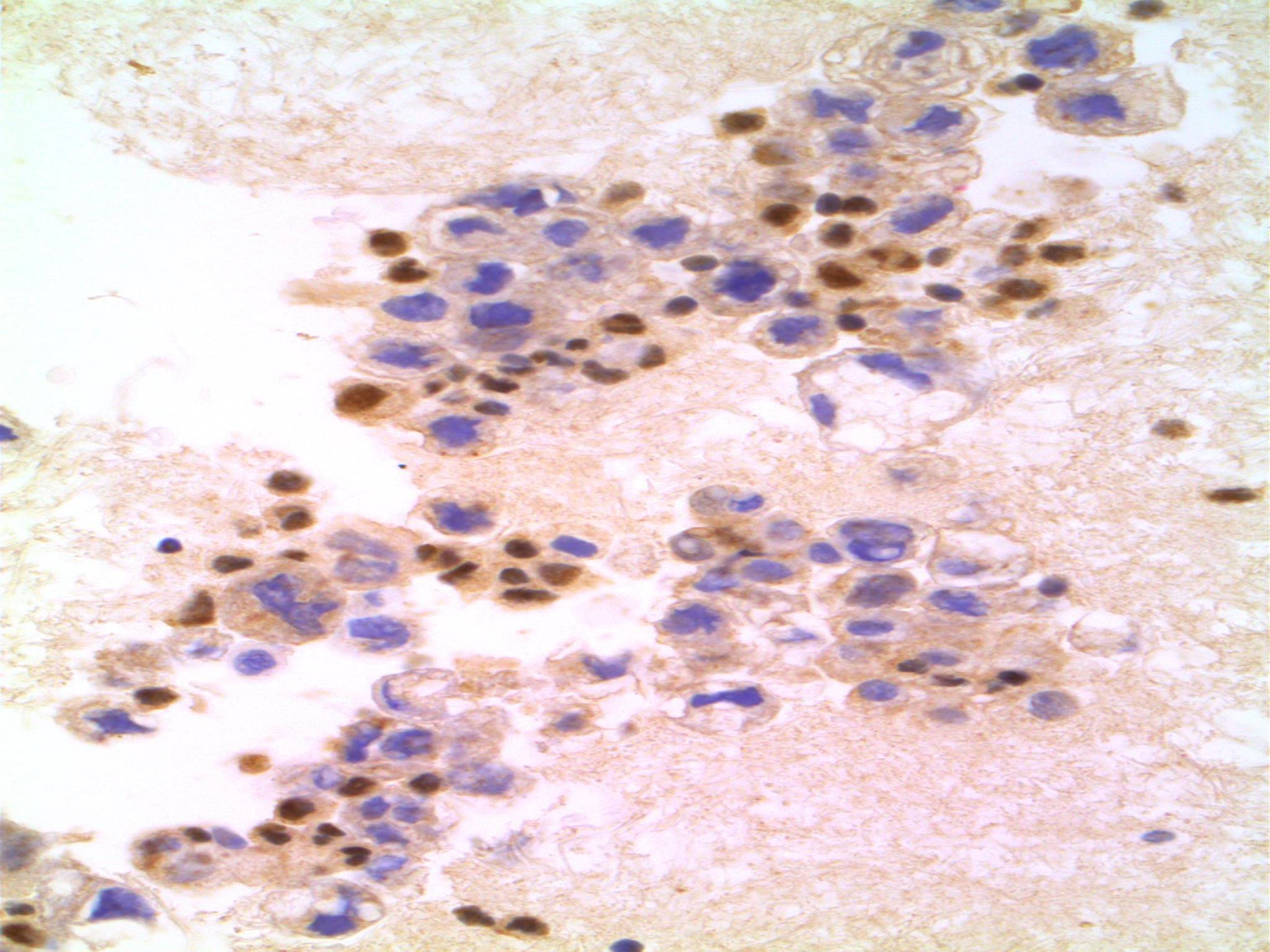 Negative immunohistochemical staining for BAP-1 with positive internal control
Negative immunohistochemical staining for BAP-1 with positive internal control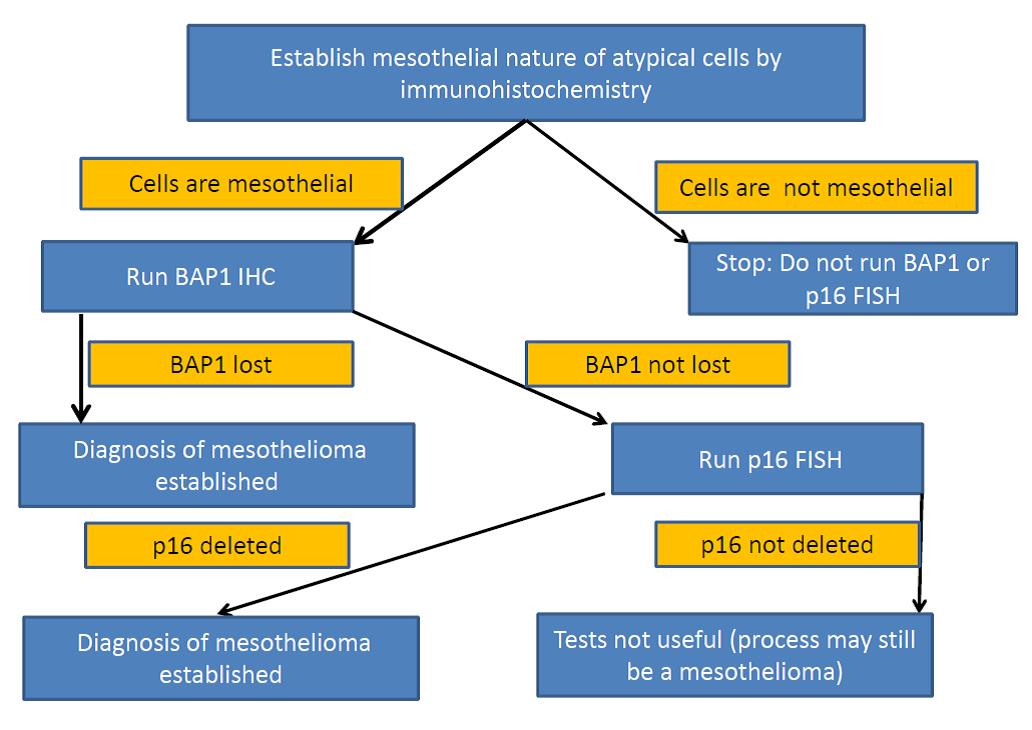
Discussion
The final cytologic diagnosis in this case was “Positive for malignant cells; consistent with malignant mesothelioma”. Subsequently, the patient had a pleural biopsy at another hospital which confirmed the cytologic diagnosis. She received chemotherapy and immunotherapy and was still alive 15 month after the diagnosis of malignant epithelioid mesothelioma but with progressive disease involving the peritoneum and pericardium (tamponade). Of note, she did not have clinical history of asbestos exposure.
In this case, the tumor cells were negative for BAP-1 (with an adequate positive internal control). This finding, combined with the cytomorphologyand immunoprofile of the tumor cells and the clinic-radiological data allowed to make a definitive diagnosis of malignant mesothelioma based on cytologic material alone (see below).
Malignant mesothelioma accounts for less than 2% of malignant effusions. It is strongly linked in most cases (up to 80%) to asbestos exposure and arises most commonly in the pleura and less commonly in the peritoneum; rarely pericardium or tunica vaginalis of the testis. Common symptoms include chest pain and shortness of breath. Most patients have an effusion, usually unilateral, at the time of presentation. Only the epithelioid and mixed (biphasic) types of mesothelioma are likely to exfoliate malignant cells; the pure sarcomatoid and desmoplastic types rarely exfoliate (1). Mesothelial proliferations can be diagnostically challenging in small specimens, such as body fluid cytology and small tissue biopsies (1,2). The main differential diagnosis includes reactive mesothelial cells, malignant mesothelioma and metastatic tumor, including mainly adenocarcinoma, squamous cell carcinoma, epithelioid hemangioendothelioma and epithelioid angiosarcoma. A great morphologic challenge for pathologists is the separation of benign reactive mesothelial proliferations from malignant mesotheliomas. Reactive mesothelial proliferations may have histologic features that resemble malignancy including increased cellularity, cytologic atypia, and mitoses. In contrast, malignant mesothelioma may lack some of these features. Therefore, classic features of malignancy (pleomorphism, high N:C ratios, hyperchromasia, prominent nucleoli, and mitoses) may not be accurate in distinguishing reactive mesothelial cells from malignant mesothelioma (1,2). In contrast, separation of mesothelioma from other malignancies is relatively straightforward using morphology and immunohistochemical stains. The choice of antibody panel to be applied in an individual case is driven by morphology, either epithelioid or sarcomatoid, and clinical history (known malignancy) (2).
Guidelines for making a cytopathologic diagnosis of epithelioid and mixed-type malignant mesothelioma in effusions require one of the following criteria (1) : • Indisputable malignant cells on cytomorphological criteria which demonstrate a mesothelial phenotype, which should be verified by ancillary techniques; • Cytomorphological features which are not unequivocally malignant, but ancillary techniques confirm malignancy and a mesothelial phenotype.
When evaluated in clinical practice, these two options can make the specific diagnosis of malignant mesothelioma with a high degree of sensitivity and accuracy (1). In cases where the material is scant and/or ancillary studies are not feasible (equivocal cases), the International Mesothelioma Panel recommends the use of a descriptive diagnosis such as “Atypical mesothelial proliferation”. In these equivocal cases, further material and diagnostic specimens can usually be obtained and bona fide malignant mesotheliomas will make themselves evident in most cases. Recent advances in mesothelioma genetics resulted in identification of BRCA-1-associated protein (BAP1) mutations and p16 deletions as features of malignant mesotheliomas (2-5). Hence, BAP1 immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) for p16 emerged as 2 most common diagnostically helpful ancillary studies that can be used on limited samples when the question is whether the mesothelial proliferation is malignant or benign.BAP1is a tumor suppressor gene, which shows biallelic inactivation in approximately half of all malignant mesotheliomas. As a result, BAP1 loss detected by IHC was reported to be a feature of malignant mesotheliomas (15-81% of cases), that is not observed in benign reactive mesothelial cells (2). Similarly, studies showed an overall sensitivity of p16 FISH in the diagnosis of malignant mesotheliomain effusion cytology across all cytologic categories of 56-79%, with a positive predictive value of 100%.While, BAP1 IHC and p16 FISH can confirm a diagnosis of mesothelioma if they are lost/deleted, failure to find loss/deletion of these markers does not make a mesothelial process benign as a significant subset of mesotheliomas do not show loss of these markers. In addition, these markers can also be lost in other types of malignancies, therefore it is essential that the pathological process is confirmed as being of mesothelial origin before applying these ancillary tests. Furthermore, the pathologic diagnosis of malignant mesothelioma continues to evolve (“doing more with less tissue”). Emerging data that indicate subtyping of epithelioid malignant mesotheliomaaccording to morphologic features and nuclear grade are important to predicting survival and suggest that a cytologic diagnosis of malignant mesothelioma epithelioid type might not be sufficientinthe future (5).
References
- Hjerpe A, Ascoli V, Bedrossian CW, et al. Guidelinesfor the CytopathologicDiagnosisof Epithelioidand Mixed-TypeMalignantMesothelioma: a secondary publication.Cytopathology. 2015;26(3):142-56.
- Monaco S, Mehrad M, Dacic S. Recent Advances in the Diagnosis of Malignant Mesothelioma: Focus on Approach in Challenging Cases and in Limited Tissue and Cytologic Samples.Adv Anat Pathol. 2018;25(1):24-30.
- Hwang HC, Sheffield BS, Rodriguez S, Thompson K, Tse CH, Gown AM, Churg A. Utility of BAP1 Immunohistochemistry and p16 (CDKN2A) FISH in the Diagnosis of Malignant Mesothelioma in Effusion Cytology Specimens.Am J Surg Pathol. 2016;40(1):120-6
- Churg A, Sheffield BS, Galateau-Salle F. New Markers for Separating Benign From Malignant Mesothelial Proliferations: Are We There Yet?Arch Pathol Lab Med. 2016;140(4):318-21
- Husain AN, Colby TV, Ordóñez NG, et al. Guidelines for Pathologic Diagnosis of Malignant Mesothelioma 2017 Update of the Consensus Statement From the International Mesothelioma Interest Group. Arch Pathol Lab Med. 2018;142(1):89-108
* Case and discussion contributed by: Marc Pusztaszeri, MD Associate Professor Department of Pathology McGill University
- 1
- 2
- 3
- Current
- Review
- Answered
- Incorrect
-
Question 1 of 3
1. Question
The MOST LIKELY diagnosis is:
CorrectIncorrect -
Question 2 of 3
2. Question
Which immunohistochemical (IHC) stain is expected to be positive in this condition?
CorrectIncorrect -
Question 3 of 3
3. Question
Which of the following genetic alteration is associated with this condition?
CorrectIncorrect