The following images are representative of a parotid gland mass fine needle aspiration. The patient is a 61-year-old male.
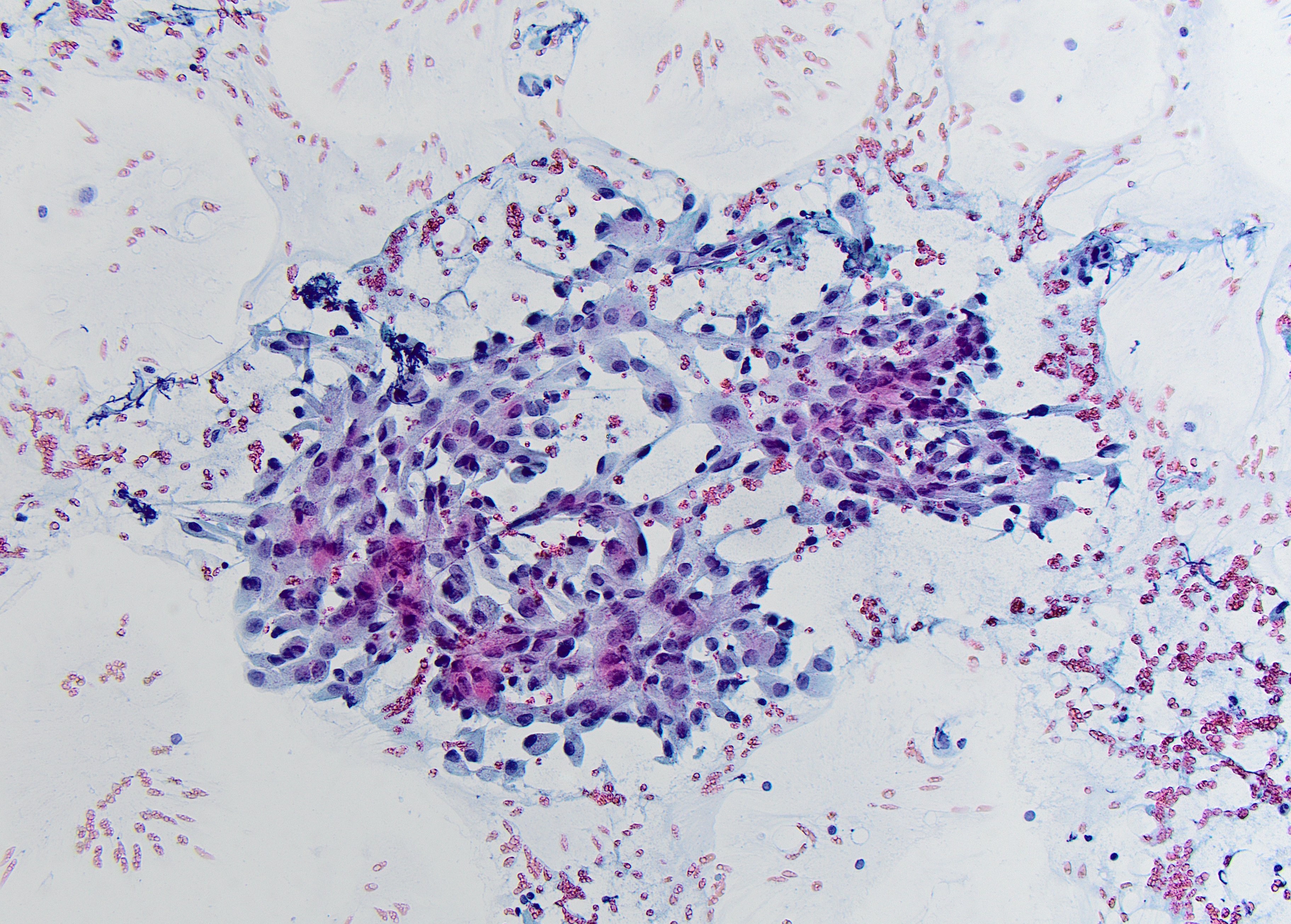
Pap stained smear x20
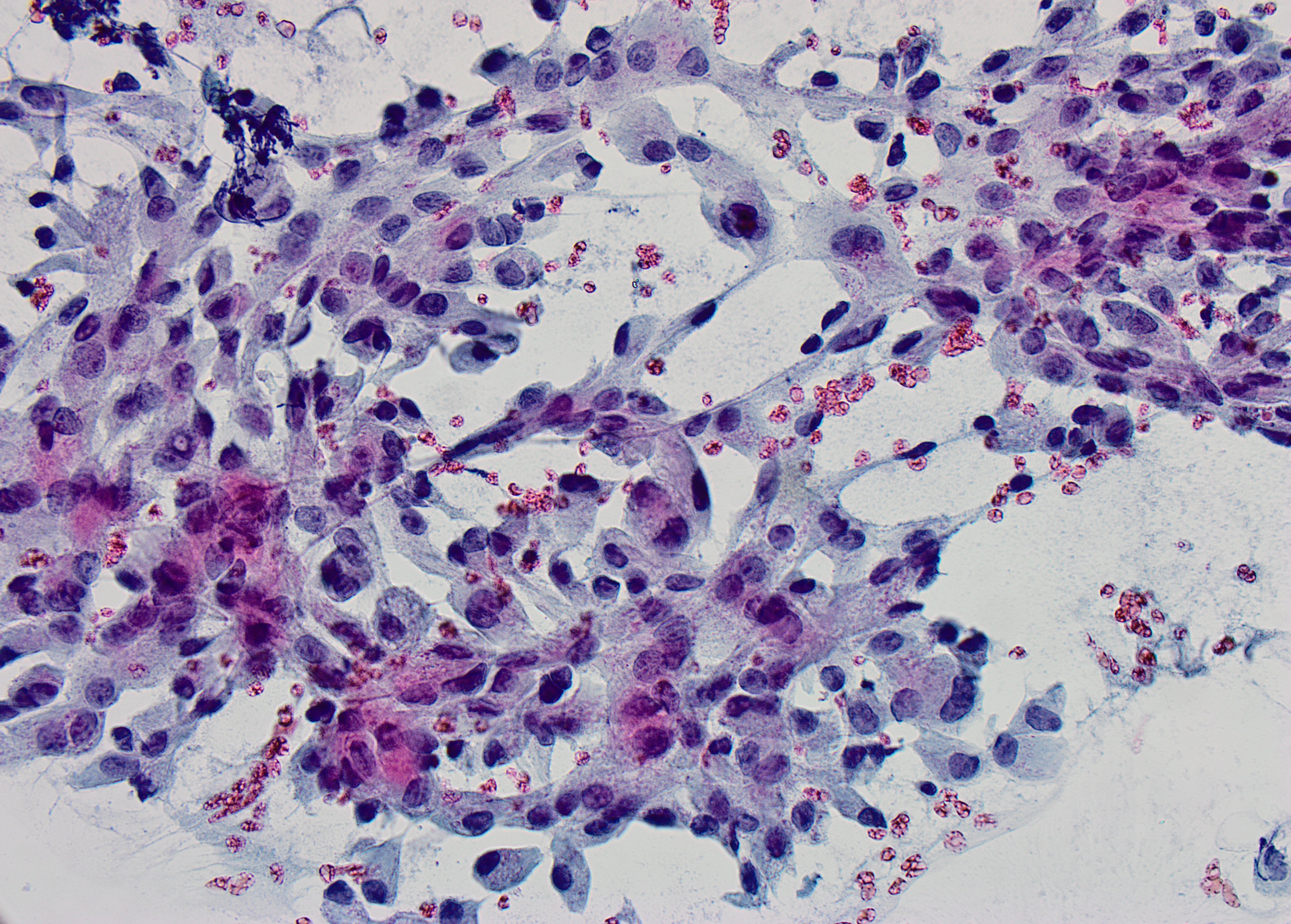
Pap stained smear x40
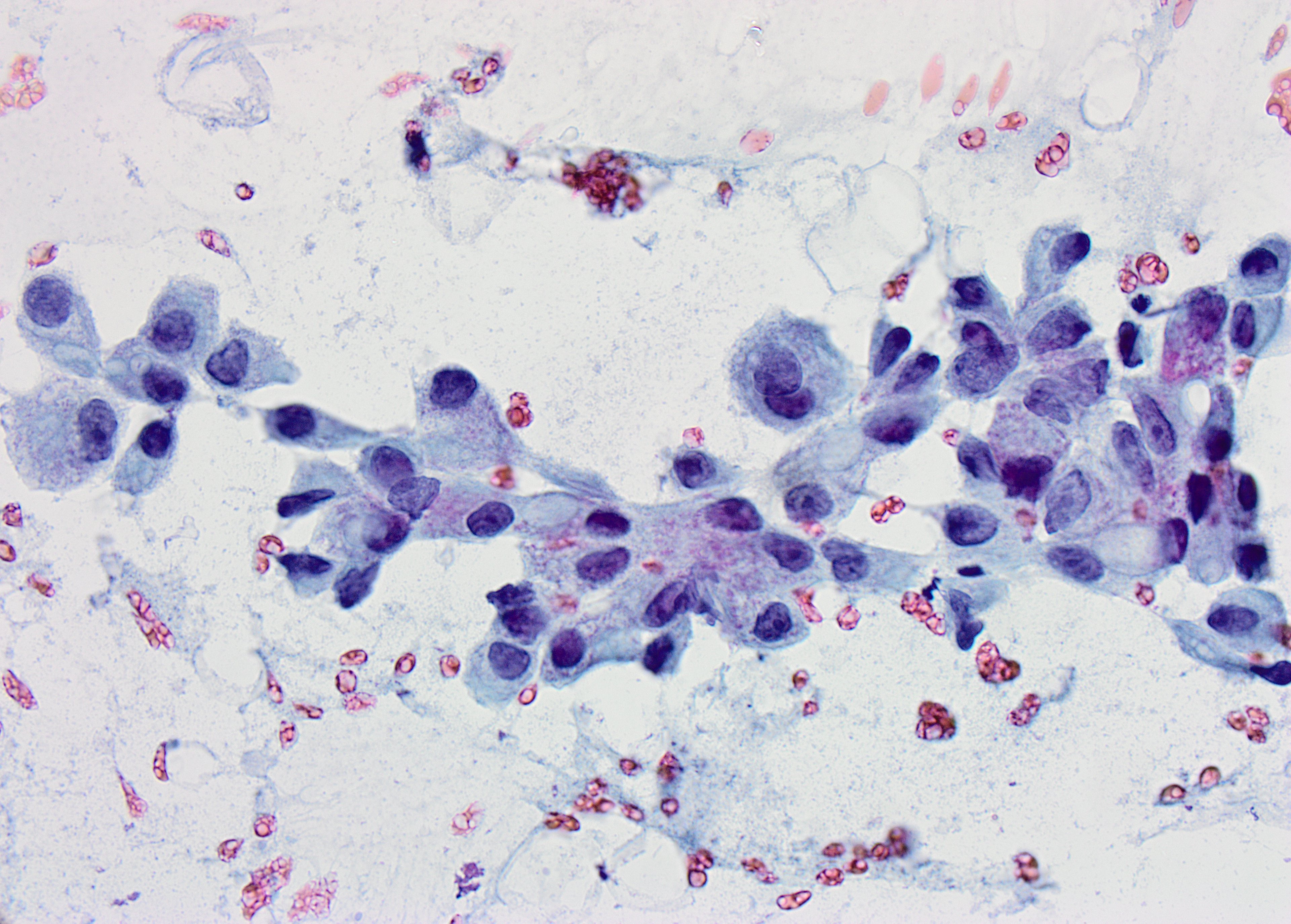
Pap stained smear x60
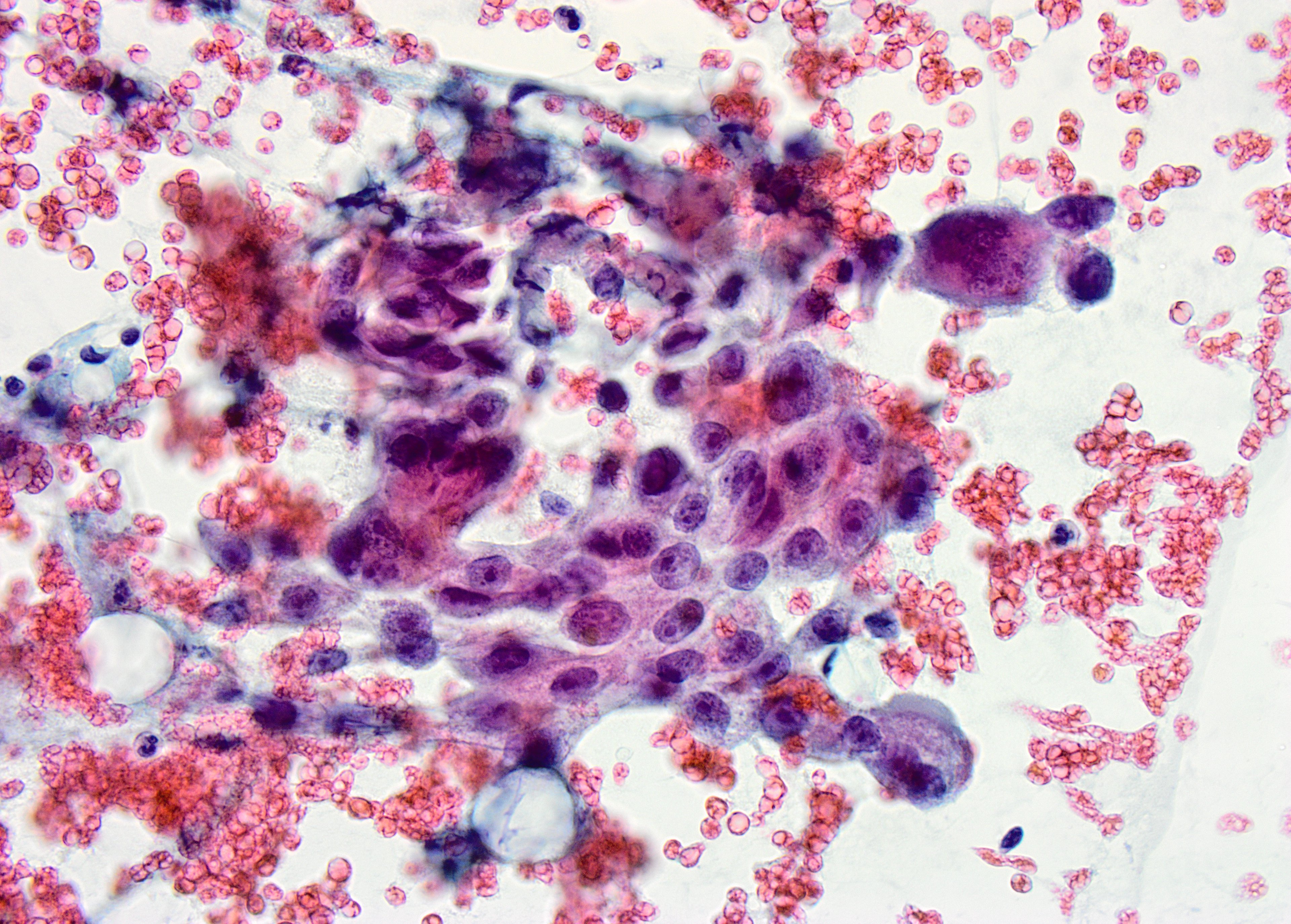
ThinPrep – Pap stained X60
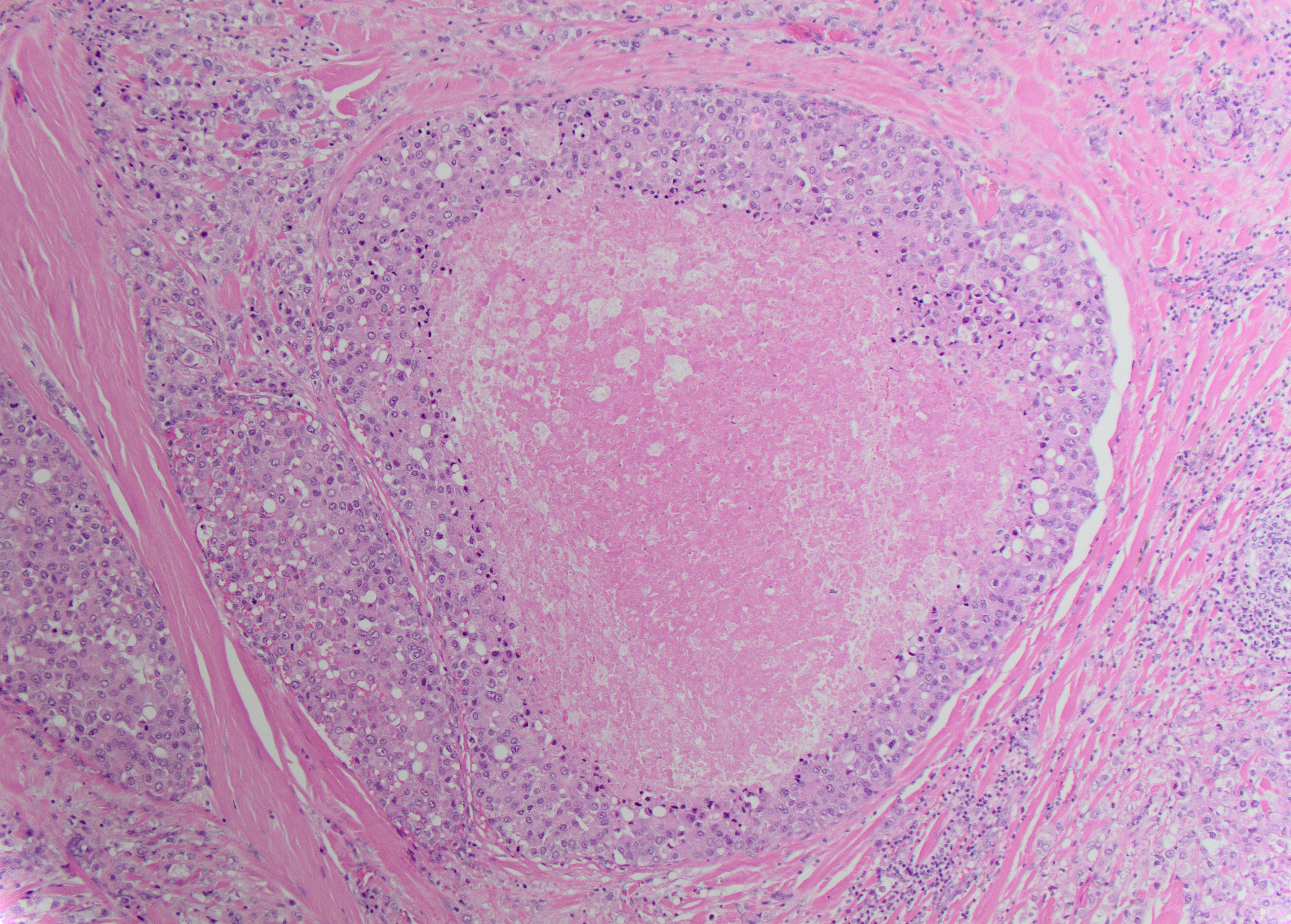
Follow up resection – H&E X10
Quiz Summary
0 of 3 questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 3 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
-
 Canadian Society of Pathology
Canadian Society of PathologyCase Of The Month
Contributor: Omar Al-Nourhji, MD, FRCPC, Assistant Professor, Department of Laboratory Medicine and Pathology, University of Saskatchewan
Glenda Wright, MBBCh General Pathology Resident Department of Laboratory Medicine and Pathology University of Saskatchewan
Flat sheet of relatively cohesive polygonal epithelial cells with ample cytoplasm and eccentrically located nuclei. The background in the image is clean with no extracellular mucin or necrosis.
Higher-power view of medium to large polygonal cells with well-defined cellular borders, relatively abundant granular cytoplasm, nuclear pleomorphism and prominent nucleoli.
The neoplastic cells demonstrate abundant granular cytoplasm with focal vacuolization, polymorphic nuclei and prominent nucleoli
A loose cluster of oncocytic cells with increased nuclear to cytoplasmic ratio, round to oval nuclei and prominent nucleoli
H&E-stained section shows a large duct with high-grade tumor cells arranged in a cribriform architecture. There is central necrosis in the gland lumen.
Discussion
Fine needle aspiration is frequently used as a first line diagnostic test in the work up of salivary gland lesions. A definitive diagnosis often can be reached based on cytomorphology alone, especially in more frequent and benign lesions such Warthin’s tumor (WT) and pleomorphic adenoma (PA). However, not infrequently, overlapping morphologic features makes ancillary studies essential in reaching the diagnosis.
The neoplasm shown in the images demonstrates an oncotyoid morphology with mild to moderate nuclear atypia and focal cytoplasmic vacuolization. Increased mitotic activity, necrosis and extracellular mucin are not identified. The differential diagnosis includes an oncoytoid mucoepidermoid carcinoma (MEC), acinic cell carcinoma (ACC), salivary duct carcinoma (SDC), oncocytic carcinoma, mammary analogue secretory carcinoma (MASC), and metastatic carcinoma (breast, lung or prostate primary). Choice (3) is the most helpful IHC panel in working up this neoplasm. DOG-1 and SOX10 are useful markers of ACC. GATA-3 and Mammoglobin are positive in MASC. P63 and mucin are positive in MEC. Choice (1) is a suggested IHC panel in the work up of basaloid salivary gland neoplasms. Choices (2) and (4) are not helpful in differentiating primary salivary gland neoplasms and are rather focused on potential metastatic diseases (renal cell carcinoma, prostate carcinoma, melanoma, etc.).
Salivary duct carcinoma is a more recently described malignant neoplasm (1), accounting for less than 10% of salivary gland tumors. It most frequently occurs in the parotid gland and presents as a rapidly growing, infiltrative mass. Cytologic aspiration specimens from SDC tend to be cellular with a necrotic background. The neoplastic cells are polygonal with well-defined cellular borders, abundant eosinophilic cytoplasm, high grade pleomorphic nuclei and prominent nucleoli (2).
Histologically, the tumor is characterized by intraductal carcinoma with characteristic “Roman bridge” architecture and central comedonecrosis and infiltrating ductal carcinoma surrounded by desmoplastic and fibrotic stroma. Almost by definition, SDCs show androgen receptor (nuclear) reactivity (3).Molecular techniques such as fluorescence in situ hybridization (FISH), reverse transcription-polymerase chain reaction (RT-PCR) and next generation sequencing (NGS) may prove helpful in establishing a diagnosis in cases with ambiguous morphology or limited diagnostic material. These techniques can be applied to various cytologic preparations (smears, liquid based preparations and most preferably cell blocks). Of the statements listed, choice (1) is the correct answer. ETV6-NTRK3 fusion gene is characteristic of MASC (4) and is reported in 90-100% of cases. PLAG1-CTNNB1 translocation is reported in 50-60% of PAs. MYB-NFIB fusion gene is associated with ACC (28-86% of cases). CRTC1-MAML2 fusion gene is identified in 60-80% of MEC.
References
- Barnes L, Rao U, Krause J, et al: Salivary duct carcinoma. Part I. A clinicopathologic evaluation and DNA image analysis of 13 cases with review of the literature. Oral Surg Oral Med Oral Pathol 1994; 78: pp. 64-73
- Mehrotra S. et al. (2018) Malignant. In: Faquin W. et al. (eds) The Milan System for Reporting Salivary Gland Cytopathology. Springer, Cham
- Fan CY, Wang J, Barnes EL. Expression of androgen receptor and prostatic specific markers in salivary duct carcinoma: an immunohistochemical analysis of 13 cases and review of the literature. Am J Surg Pathol. 2000;24:579–586
- Skalova A, Vanecek T, Sima R, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34:599–60
* Case and discussion contributed by: Omar Al-Nourhji, MD, FRCPC, Assistant Professor, Department of Laboratory Medicine and Pathology, University of Saskatchewan
- 1
- 2
- 3
- Current
- Review
- Answered
- Incorrect
-
Question 1 of 3
1. Question
Which immunohistochemical (IHC) stain panel would be MOST HELPFUL to establish a diagnosis?
CorrectIncorrect -
Question 2 of 3
2. Question
The cell block from this specimen is reported to have positive IHC staining for Androgen receptor. What is the CORRECT diagnosis?
CorrectIncorrect -
Question 3 of 3
3. Question
Which of the following statements regarding molecular findings in salivary gland neoplasms is CORRECT?
CorrectIncorrect